



INTRODUCTION
Osteoporosis, the most common metabolic bone disease, is defined as a systemic skeletal disease that causes an increase in bone fragility as well as fracture risk as a result of impaired bone micro-architecture and low bone mineral wear.[1] With the increase in the frequency of osteoporosis with age, fractures associated with osteoporosis are seen in one-third of the female and one-fifth of the male sex after the age of 50.[2] The global prevalence of osteoporosis among individuals aged 15 to 105 years is estimated at 18.3%.[3] Osteoporosis is a silent disease until complicated by fractures that may occur following minimal trauma or, in some cases, without trauma.[4] Osteoporosis and accompanying fractures increase mortality and morbidity, especially when they occur in the hip and spine regions.[5] Given the aging of the world’s population, it’s clear that the osteoporosis problem is likely to get bigger by the day. For this reason, it is extremely important to identify risk factors, have sufficient knowledge about osteoporosis, develop a sense of self-efficacy, implement necessary life changes, develop preventive practices by raising awareness, and make early diagnosis.[6] Osteoporosis and its associated morbidities have received considerable attention as a public health problem and economic burden.[7] In light of all this, preventing this disease can significantly reduce the costs incurred by the healthcare system.[8]
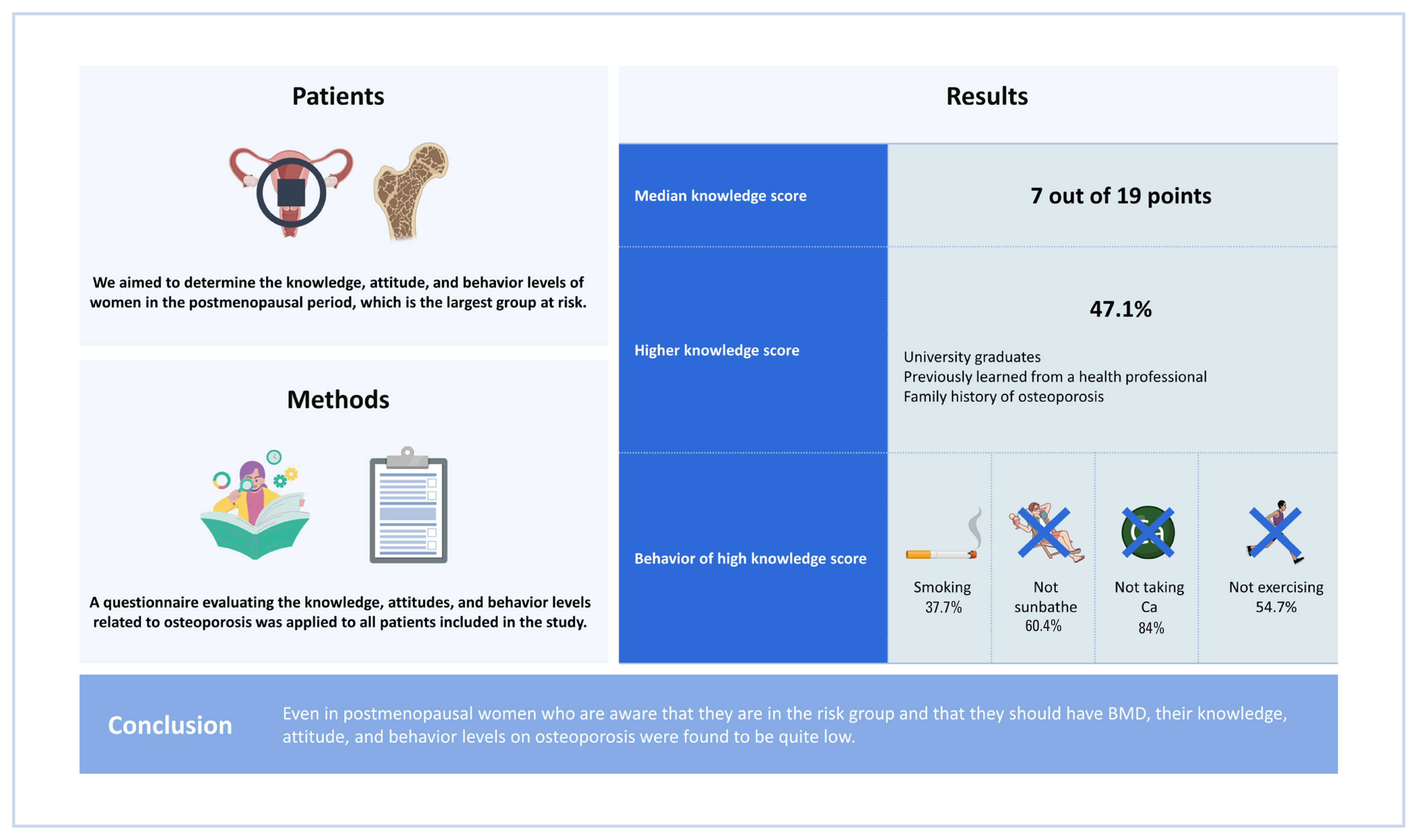
Although it has been shown that osteoporosis knowledge and health beliefs have a positive effect on preventive measures and screening rates, the number of such studies in the Turkish population is insufficient. İn a study comparing the knowledge and awareness levels of pre- and post-menopausal women, it was found that there was no difference between the 2 groups.[9] In a study conducted in Turkey in 2014, the knowledge and awareness levels of men and women about osteoporosis were compared, and it was shown that there was no difference.[10] Therefore, in this study, we aimed to determine what the deficiencies are by determining the knowledge, attitudes and behaviors of patients who come to the tertiary hospital for osteoporosis in the postmenopausal period.
METHODS
The study was conducted between December 1, 2018 and May 1, 2019, at the tertiary care Training and Research Hospital’s Family Medicine outpatient clinics in Ankara, where bone mineral density (BMD) measurements were performed. The study included postmenopausal women who either applied for BMD measurement or had previously undergone this measurement at least once and agreed to participate. All individuals with mental retardation problems, speech and language problems, and female individuals who are not in the menopausal period were excluded. In the study, 225 postmenopausal women were administered a questionnaire prepared by the researchers and evaluated their knowledge, attitude and behavior levels about osteoporosis. The questions included in the questionnaire included positive and negative behaviors to assess their relationship with osteoporosis. While regular exercise, calcium consumption, and sunbathing were questioned as positive behaviors, parameters such as smoking, alcohol use, sedentary life habits, and nutritional mistakes were among the negative behaviors.
Statistical analysis
Data analysis was done with SPSS 25.0 software (SPSS Inc., Chicago, IL, USA). In the study, the relationship between the knowledge and attitude levels and the variables was determined by the χ2 test; the relationship between the calculated scores and the frequency of use of foods with the Pearson correlation test; The differences in scale scores according to demographic variables were analyzed by independent groups t-test and ANOVA tests.
RESULTS
The mean age of the women participating in the study was 58.05±9.1 years and the mean body mass index was 29.53±5.06 kg/m2. About 35.1% of the individuals had a high school education and above, and 36% were primary school graduates. Participants 67.6% of them were housewives. A family history of osteoporosis was present in 35.6% of the women, and 80.4% had previously learned about osteoporosis. Information about osteoporosis was mostly (34.3%) obtained from mass media such as newspapers, TV, and the internet (Table 1).
In order to evaluate the knowledge level of the individuals participating in the study about osteoporosis, 19 questions were posed. Considering the answers given by the individuals to the questions, their knowledge status was evaluated (Table 2). The mean knowledge score was found to be 7.19. Median (7) value and above point fields high rated low fields whereas low rated groups aspect determined. It was observed that 52.9% of the participants had a low level of knowledge. When osteoporosis knowledge scores were evaluated according to the prepared questionnaire, it was determined that the median scores of those who had a family history of osteoporosis, those who were university graduates, who were previously informed about osteoporosis by a healthcare professional and those under the age of 45 were significantly higher than those of other people.
The mean attitude score was 9.44, the median value was 9, and 52% had a low attitude level. Considering the behavior of those included in the study towards the osteoporosis; 66.7% of them did not smoke and 90.2% of them did not use alcohol. About 36.9% of women were exercising occasionally, 64.9% were walking mostly, 49.8% were exercising less than 30 min. Twenty-eight percent of the women were taking calcium supplements and 45.3% were taking vitamin D supplements. About 31.6% of the individuals participating in the study were injured by the sun’s rays every day, and the skin of 44.9% was in contact with the sun’s rays for less than 1 hr. Sixty two point two percent of individuals drank 1 to 2 servings of milk, 12.4% were using drugs that reduce BMD (Table 3).
We evaluated individuals based on certain osteoporosis-related behaviors, standings, and prior knowledge of the osteoporosis. People with high knowledge scores smoked more than those with low knowledge scores. The osteoporosis knowledge level of individuals who regularly sunbathed every day was higher. The level of knowledge of individuals consuming 3 to 4 servings of milk and dairy products per day was similarly significantly higher.
DISCUSSION
In our study, it was found that 52.9% of postmenopausal women had low level of knowledge, 80.4% had received information about osteoporosis before, 36.9% exercised occasionally, 35.6% had a family history of osteoporosis, 62.2% consumed 1 to 2 servings of milk and dairy products. It is very important for women in the postmenopausal period to be protected from osteoporosis and the complications of the disease. Preventing the formation of osteoporosis by taking the necessary precautions before it occurs is closely related to increasing the knowledge and awareness levels of postmenopausal women, especially the target group.
Osteoporosis is a public health problem that can be delayed or even prevented by measures such as lifestyle changes. Since it can show an asymptomatic course for a long time, it is possible to prevent possible complications if risk factors are questioned in the early period and BMD measurements can be made on time. Estrogen deficiency developing during and after menopause causes a decrease in BMD. The incidence of osteoporosis in women over 50 years of age in the USA was 15.8%.[11] In our study, the rate of patients who were diagnosed or declared to have osteoporosis was similarly found to be 19.1%.
It was determined that 52.9% of the participants had low level of knowledge. When the literature was examined, it was seen that similar results were found.[12-16] In addition to these studies in which osteoporosis knowledge was found to be insufficient, other studies with high or moderate osteoporosis knowledge took their place in the literature.[17, 18] The results of these studies differ from our study. It was thought that their high awareness about osteoporosis might be related to their education level. In our study, there was a statistically significant difference among women with different educational status in terms of osteoporosis knowledge score. While the osteoporosis knowledge level of university graduates is the highest, illiterate students are the lowest. The results obtained from similar studies support this argument.[18-20] In our research questionnaire, participants were asked whether they had received information about the osteoporosis before. The 80.4% of the participants stated that they received information. When the information sources questioned it was seen that the answer of 34.3% was mass media such as newspaper, television, Internet. The rate of those who obtained the information from the health personnel took the second place as 30.9%. Studies conducted in West India and Lebanon have also determined that the most common source of information about osteoporosis is the media.[12,15] In our study, there was a significant difference in terms of osteoporosis knowledge score among women who had different sources of information about osteoporosis. Those who received information from health personnel had the highest level of osteoporosis knowledge, while those who received information from relatives and friends had the lowest score. From this point of view, it is an undeniable fact that it is necessary for doctors and other health personnel to inform about osteoporosis and to reach wider masses.
Of the individuals participating in our study 33.3% were smoking and 9.8% were using alcohol. It was observed that the osteoporosis knowledge level of those who smoked more than 20 cigarettes a day was the highest with 70%. This surprising result made us think that the group who scored high on the osteoporosis knowledge test could not transform the knowledge they acquired into behavior. In a study conducted in India, an osteoporosis knowledge assessment questionnaire was administered to postmenopausal women and the results showed that 66.7% of the participants were not aware that smoking may contribute to osteoporosis.[12] In the light of all these, it is obvious that it is difficult to inform the public about the osteoporosis and to reflect on the attitude and behavior.
Physical activity prevents the development of osteoporosis by providing peak bone mass formation in young individuals and by protecting existing bone tissue in elderly individuals. It has been proven that daily regular physical exercises have positive effects on skeletal health, while sedentary life and inactivity lead to bone tissue loss.[21,22] In our study, it was determined that 36.9% of the participants exercise occasionally, and 64.9% of them preferred walking the most. The 49.8% stated that they exercised less than 30 min. In a study by Ahmadieh et al. [13], it was shown that participants had low rates of exercise and were unaware of the benefits of exercise in preventing osteoporosis. In 2 other studies, it has been shown that training and incentives to be given to individuals in order to regularly apply isometric exercises to prevent the development of osteoporosis will be effective.[23,24] There was a family history of osteoporosis in 35.6% of the participants in our study. In a study conducted in India, it was found that 59% of the participants were aware that the presence of a positive family history increased the risk of developing osteoporosis.[12] In a cross-sectional study conducted by Ahmedieh et al. in 2018 [13], it was noted that half of the participants, and in the study conducted in Turkey, 74.8% of the participants knew that family history constitutes a strong risk factor for osteoporosis.[13,16] In our study, the rate of people who knew that the presence of osteoporosis in the family was a risk was 51.6%. In addition, it was determined that the osteoporosis knowledge level of women with osteoporosis in their family was significantly higher.
Nutritional habits have an extremely important place in preventing osteoporosis. Calcium and vitamin D deficiency, especially in postmenopausal women, results in decreased BMD. This will cause bone loss and fracture. It is possible to provide the needed calcium supplement by consuming sufficient milk and dairy products. According to the 2022 TEMD guidelines, it is recommended that a postmenopausal woman take 1,200 mg of calcium daily. The daily requirement must be obtained primarily through nutrition. About 62.2% of the participants in our research stated that they consume 1 to 2 servings of milk and dairy products. Twenty one point eight percent of them said that they almost never consume these foods with rich calcium content. This ratio does not meet the required amount of calcium. However, only 28% of women take calcium supplements. The 45.3% stated that they took vitamin D supplements. In a study by Senthilraja et al. [12], it was determined that 65% of the participants were aware that milk is an important source of calcium. In a study of women over 50 years of age, 81% of participants indicated that they thought calcium-rich diets were helpful in preventing osteoporosis. The 78% were aware that vitamin D levels were a risk factor for developing osteoporosis.[13] When a selected group of medical professionals living in Southern India were asked through a questionnaire what the calcium and vitamin D levels needed to prevent osteoporosis were, only 61.4% were able to answer correctly.[25] In a study examining the knowledge and behavior levels of osteoporosis in women with premature ovarian failure and early menopause, it was found that 99% of the participants had serious knowledge gaps about calcium intake and diet.[26] Similar to the literature, in our study, we found that there is a significant relationship between the daily consumption of milk or dairy products by women and the level of osteoporosis knowledge. It has been observed that those who consume 3 to 4 servings of dairy products per day have a high level of attitude and behavior related to osteoporosis.
Those who participated in our study 31.7% of them are sunbathing every day, 59.4% of them are benefiting from sunlight at least 2 to 3 times a week, while 16.5% of them are almost never sunbathing. Frequency of exposure of exposed parts of their body to sunlight showed significant differences among different women in terms of osteoporosis knowledge score and attitude score. The level of knowledge and attitude of the participants who came into contact with serious sun rays every day was found to be the highest. In addition, it was observed that 90.2% of the individuals knew that the contact of the body with the sun’s rays is important in protecting from osteoporosis. In a study by Ahmediehy et al. [13], it was determined that 85% of the participants knew that sunlight is a source of vitamin D. On the other hand, in a study conducted with 546 women, 83.9% of whom were non-health professionals and 16.1% were health workers, in Saudi Arabia, it was seen that both study groups did not have a satisfactory level of knowledge about the effect of sunlight exposure on the development of osteoporosis.[27] However, in many studies, it has been proven that direct contact of the sun with the skin has a positive effect on the synthesis of vitamin D, which is very important for skeletal health.[28,29] For this reason, taking into account the hours of the day and for how long, the importance of sunbathing correctly and adequately for bone health should be conveyed to individuals, and awareness should be increased and it should be encouraged to become a behavior.
CONCLUSION
According to the results of our study, it is necessary to raise awareness about osteoporosis, which is an important public health problem.
The role of preventive medicine practices in preventing the development of the disease is extremely important. Raising awareness of the society is the first step so that parameters such as nutrition, exercise and benefiting from sunlight can become a lifestyle. It is extremely difficult to improve the attitudes and behaviors related to protection from osteoporosis in societies with low level of knowledge. At this point, a great responsibility falls on all health personnel, physicians, especially family physicians who are responsible for providing preventive health services. Considering that physicians working in primary care are constantly providing health services to the same population and for a long time, it is clearly seen that they play a very important role in raising awareness of osteoporosis and raising public awareness.
The main service options are to inform women, to carry out protection studies, to provide training and to identify risk groups and contribute to the solution through screening.
Today, it is possible to increase awareness by providing accurate, up-to-date and effective information that can be easily accessed by everyone through these channels in terms of the large population addressed by mass media such as radio, television and the internet. However, while doing this, experts should be taken as a reference and it should be checked whether the correct information is transferred.
 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Print
Print






