


INTRODUCTION
Changes in household composition due to economic growth and alterations in social structure of Korea have resulted in a steady decline in the number of household members.[1] From 1990 to 2005, the 4-person household was the major household type; however, in 2010, the rate of 2-person households increased, and from 2015, the rate of single-person households has increased significantly.[2]
The Statistics of Korea define single-person households as individuals living alone in general households i.e., households where a single person is sleeping, cooking, and living independently.[3] These single-person households are affected by economic factors such as unstable employment, low income level, and expansion of employment for women as well as by social factors such as high education level, increasing age at the time of first marriage, increase in divorce rate, increase in individualism, changes in marriage, and rapid aging.[4,5] It is rapidly increasing due to various factors. In particular, the number of elderly people aged 65 years or older who live alone is rapidly increasing due to population aging.[6]
Increase in the number of single-person households has resulted in many changes in diet as well as social environment, such as the increasing reliance on processed and instant foods and nutrient imbalance.[7,8] In case of the elderly population, social support is an important factor [9] because they find it difficult to prepare or purchase a meal on their own and they may feel lonely. Therefore, nutrition consumption differed significantly between elderly people living with family members who prepare their meals and elderly people who live alone; elderly people living alone were more likely to be exposed to nutritional risk than elderly people living with family members.[10] A study that compared between single-person households and family households reported that intake of protein-rich foods and fruits was low among single-person households [11] and households with several members; another study reported that presence or absence of a spouse affected food intake.[12] In addition, a high rate of eating breakfast and eating out alone whereas a low rate of fish and seafood consumption was reported.[11] According to a previous study on health status of household members according to type of household, elderly people living alone had more than one chronic disease; a single elderly person was less healthy compared to an elderly person living with their family. They also showed poor health behaviors related to obesity, drinking, and smoking.[13]
Rapid aging of the Korean population and increase in number of single-person households will continue in the future; thus, an in-depth analysis is highly needed. The purpose of this study was to analyze the dietary and health status of elderly people according to type of household and to provide basic data for effective management of health-related problems.
METHODS
1. Study subject
This study used data from the Korea National Health and Nutrition Examination Survey (KNHANES) conducted from 2013 to 2014. Of the total subjects, the data of only men and women aged ≥65 years were first extracted (n=3,562), and that of only 2,730 subjects were analyzed after excluding the subjects who had missing values for multiple variables (n=832). The type of households was classified as one family member when the number of household members was one and family accompanying family members when 2 or more family members were used.
2. Study variables
In gender, age, household income (low, middle-low, middle-high, high), region (urban, rural), marriage status (married, unmarried) and education level (elementary school or below, middle school, high school, university or above) were used as socioeconomic data in the KNHANES. We used the results associated with smoking and alcohol consumption, activity limitation, subjective health status and quality of life (QOL) and analyzed the comorbid conditions of the subjects such as obesity, hypertension, diabetes mellitus, dyslipidemia, arthritis, stroke, myocardial infarction and renal failure.
Nutrient intake status was analyzed based on the survey data. Index of Nutritional Quality (INQ) of protein, calcium, phosphorus, iron, sodium, potassium, vitamin A, thiamin, riboflavin, niacin and vitamin C were calculated based on Dietary Reference Intakes for Koreans.[14] INQ is an index that evaluates the degree of satisfaction of each nutrient with sufficient energy intake. A value of 1 or more means that the quality of the meal is good. A value of less than 1 means that the nutrient intake is insufficient. In the KNHANES, food insecurity assessments use food instability items in the US National Health and Nutrition Survey. The food insecurity was compared according to the household type.
3. Statistical analysis
The mean and standard deviation (SD) were calculated using SPSS software program version 18.0 (SPSS Inc., Chicago, IL, USA). All data were reported as mean±SD or as numbers and percentages. Groups comparisons used χ2 tests for qualitative variables and independent t-test for quantitative variables. All results were considered statistically significant when P<0.05.
RESULTS
1. Demographic factors of the subjects
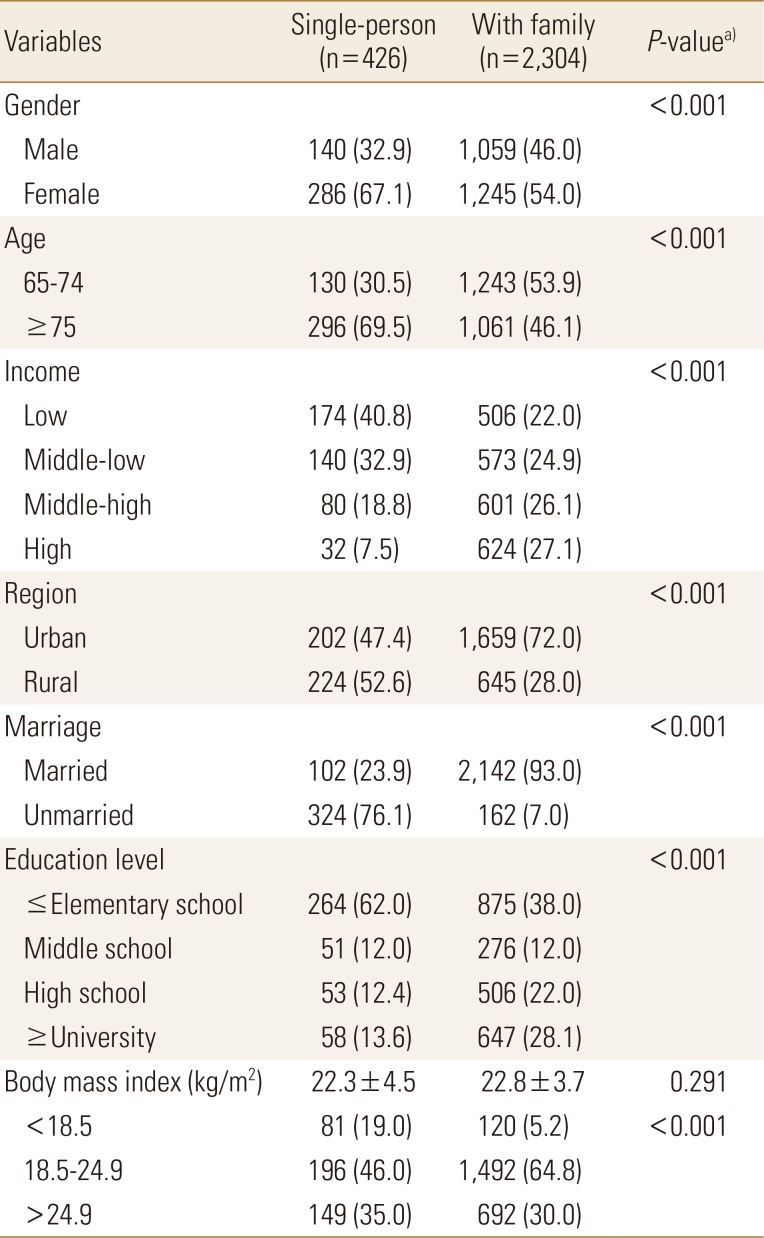
Of the total 2,730 respondents, 426 (15.6%) lived in single-person households. The proportion of female in the single-person households was significantly higher than that of family households (P<0.001). The proportion of low economic level, rural residence, and low education level was also significantly higher among people living in single-person households than among those staying in family households (P<0.001) (Table 1).
2. Disease status and health behavior factors of the subjects
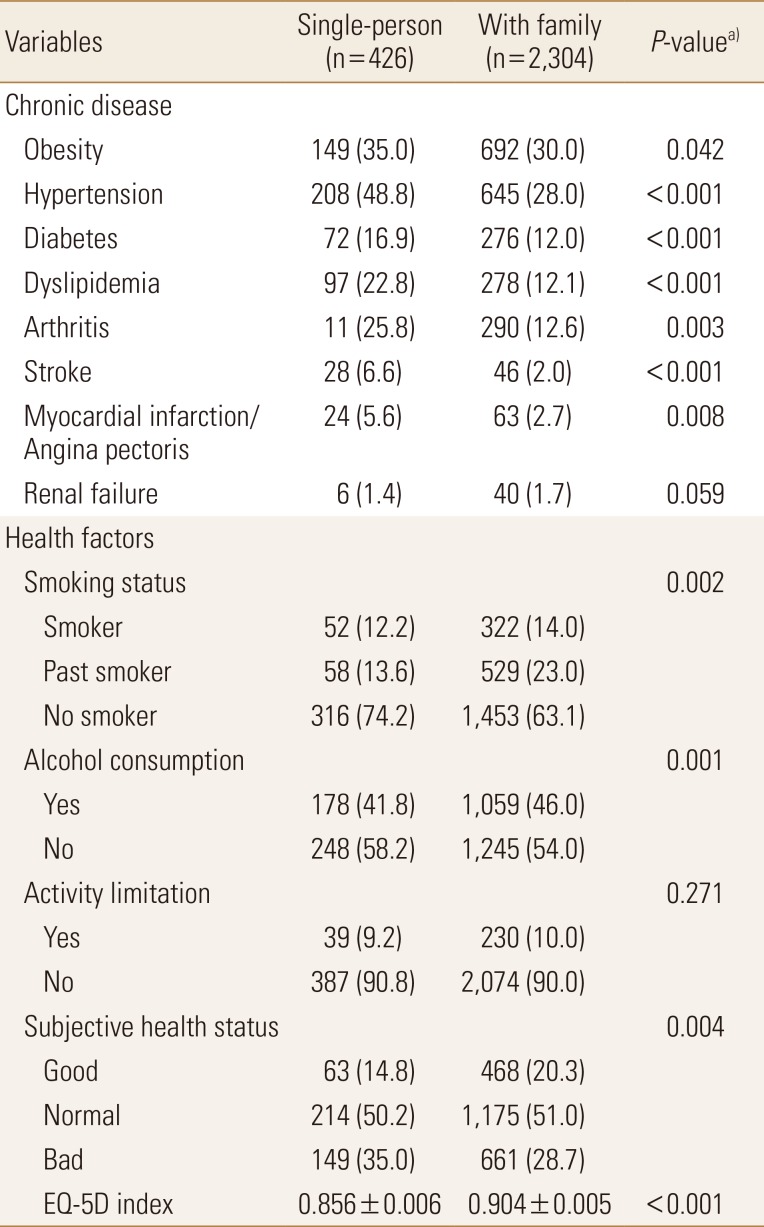
All variables related to chronic disease except renal failure were significantly different between the 2 groups. People living in single-person households had a higher prevalence of obesity, hypertension, diabetes, dyslipidemia, arthritis, stroke, and myocardial infarction than people living in family households. On evaluation of subjective health status perception, a high percentage of respondents from the single household group said that they were not healthy; the score of QOL was significantly lower in the single-person household group than in the family household group. There was no difference between the 2 groups in terms of activity limitation (Table 2).
3. Nutritional quality of the subjects
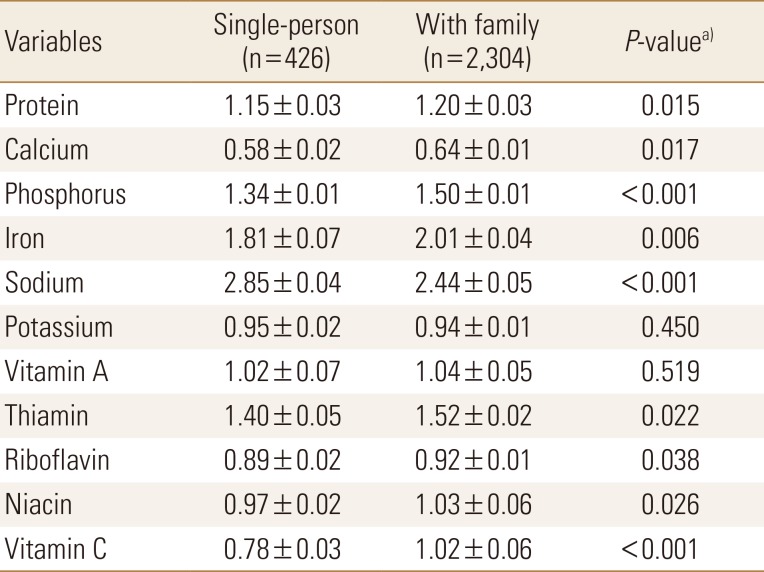
Nutrients with a lower quality of intake were analyzed. Calcium, potassium, riboflavin, niacin, and vitamin C intakes were low in single-person households; calcium and riboflavin intakes were low in family households. In particular, calcium and riboflavin were the common low-intake nutrients in both groups (Table 3).
4. Food insecurity of the subjects
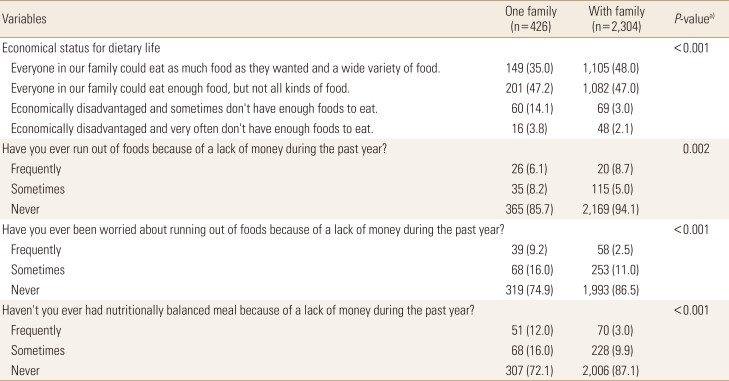
Results of food insecurity showed that the rate of eating various foods as desired was low among people living in single-person households. Furthermore, the percentage of not eating enough food frequently due to economic difficulties was significantly higher in single-person households than in family households. The percentage of respondents who did not buy food because they did not have enough money in the past year and the percentage of people who were worried about buying food were significantly higher in single-person households than in family households. In addition, the proportion of being unable to eat a nutritionally balanced diet was significantly higher among people living in single-person households than among those living in family households (Table 4).
DISCUSSION
In Korea, due to social problems such as nuclear family, increase of economic activity of women, marital avoidance phenomenon, and population aging, the number of single-person households has increased, and the type of household has been diversified and dietary problems have been raised. Therefore, in this study, we tried to analyze the health and dietary status of the elderly by using the data of the 6th KNHANES (2013-2014). The proportion in single-person household was higher for women, older people, unmarried people, and lower economic and income levels. In the previous studies analyzing the characteristics of households, the unmarried ratio of single male household was high and the low income ratio was high in single female household.[15] Although this study did not compare gender, it may have been influenced by the slightly higher proportion of women in this study.
There were many differences in the comparison of the disease status and health status according to household type. The prevalence of chronic diseases was higher in single-person households, which is the same as in the previous study.[13] In the Won and Choi [16] among the single-person households, the young people reported that their health status was better and the gap was the largest in the middle-aged. The rate of people who think that single-person household is unhealthy is higher and the death rate is higher.[17] In a study of elderly people, the number of chronic illnesses and the rate of 2 or more diseases were significantly higher in single-person household.[18] A single-person household is more likely to have polarization, aging, and femininity than general households.[19] Therefore, adults who live alone in an overly competitive society are exposed to various health problems caused by poor health habits such as irregular life, unbalanced diet, excessive stress, smoking and drinking.
In the survey on health behavior, the low smoking and drinking rate is due to the high percentage of women in this study. The perception of health and the QOL were lower in single-person households. The QOL is influenced by factors such as economic income, health level, and psychological status. It seems reasonable that the QOL is low because single-person households was poor than the family households.[20]
A comparison of nutritional quality indices revealed that the nutrient intake of single-person household was inadequate. The intake of sodium was excessive and the intake of calcium and riboflavin was particularly insufficient. This was similar to the previous study in which vitamin D, riboflavin, and calcium in the elderly were inadequately consumed.[21] The elderly often prefer to salty food, a high carbohydrate intake, and maintain a diet that lacks calcium intake. Most single-person households do not purchase food, but most of them have a high rate of eating out or buying cooked food. In addition, the regular meal rate was low and satisfaction of their diet habit was low.[22]
In the survey on food insecurity, it was found that 14.1% of single-person households did not eat enough food sometimes due to economic factors, and 3.7% of them did not often eat food. There was also a higher rate of having worried about eating food without eating it because it lacked money. In other studies, it was reported that the lower the food stability, the lower the nutrient intake and the higher the energy density, and the effective factor influencing the food insecurity was the household income.[23] In other studies, the intake of vitamins and minerals was lower in single-person household and the nutrient intake was affected by the season in the elderly group.[12]
The reason for the higher food insecurity of single-person households compared to those living together is that they are responsible for the economic burden alone. Therefore, single-person households with low income are more likely to experience food insecurity.
This study has some limitations. First, the causal analysis of the factors affecting the health of single-person households was not conducted and only cross-sectional analysis was conducted. The age and sex of the subjects were not subdivided into multiple angles. It is also regrettable that age-specific comparisons were not performed because only the elderly were analyzed. A comparative study of insufficient food intake and sarcopenia is also expected to be conducted in the future. However, it has significance in analyzing the national health statistics of Korea and analyzing the health and nutritional status of the elderly living alone.
 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Full text via PMC
Full text via PMC Download Citation
Download Citation Print
Print






