



INTRODUCTION
Spinal muscular atrophy (SMA) is a group of rare inherited neuromuscular disorders with an incidence of around 10 in 100,000 live births.[1] It is caused by mutations in the survival of motor neuron 1 gene (SMN1) and is characterized by progressive muscle weakness and muscle atrophy. Childhood-onset SMA is classified into 3 subtypes based on the age of onset and best motor function achieved, with SMA type 1 being the most severe form (onset before the age of 6 months and non-sitter) and type 3 being the mildest form (walker but progressive muscle weakness after the age of 18 months).[1]
In the past, bone health was often a neglected issue in the care of children with SMA. However, osteoporosis is indeed a common problem, and fractures have been reported to be highly prevalent at up to 38% of these children.[2] This is attributed to both immobility and the functional role for SMN protein in bone remodelling.[2,3] In fact, bone health is one of the key factors determining the quality of life of patients with SMA. Therefore, in recent years, bone health assessments have been highlighted as a crucial part of SMA management.[4] Moreover, with the emergence of various effective disease-modifying treatments, including nusinersen and risdiplam, the natural course of the disease has been transformed.[5] Therefore, to maximise the effect of these treatments, it is important to prevent and manage its associated comorbidity, including osteoporotic fractures.
The objective of the study is to evaluate the bone health status in children with SMA in Hong Kong.
METHODS
This is a retrospective study. Children with molecularly confirmed SMA, who were managed in 2 quaternary centers, Queen Mary Hospital and Hong Kong Children’s Hospital from 1st April 2021 to 31st March 2022, were recruited.
Their demographic data and clinical information, including SMA types, current ambulatory status, history of fractures, vitamin D status, bone mineral density (BMD), as well as drug treatment were retrieved from electronic medical records. Their bone health status and factors associated with compromised bone health including SMA types and ambulatory status were analysed.
The study was approved by the Institutional Review Board of the University of Hong Kong/Hospital Authority Hong Kong West Cluster and Hong Kong Children’s Hospital Clinical Research Ethics Committee.
1. Diagnosis of SMA
The diagnosis of the children with SMA participating in this study was confirmed by molecular testing with homozygous deletion in SMN1 in an accredited genetic diagnostic laboratory. All patients had a classical SMA phenotype with verification by the attending pediatric neurologist (SHC). Ambulatory statuses were categorized as ‘walker’, ‘assisted walker’, ‘sitter’, ‘assisted sitter’ and ‘non-sitter’.[6]
2. Bone health assessment
Areal BMD (aBMD) was measured by dual energy X-ray absorptiometry (DXA) using the Hologic Horizon A system (Hologic Inc., Bedford, MA, USA) at the total body less head (TBLH), postero-anterior lumbar spine (LS) and/or lateral distal femur (LDF),[7,8] depending on whether patients had any metallic implants or fixed contractures that would affect the scanning results and positioning. Calculations of Z-scores and height-adjusted Z-score were based on published reference data.[9] Collapsed vertebrae, if any, were excluded from aBMD measurement. Data on patients’ last DXA measurement were collected and analysed.
A low BMD for age was defined as a BMD Z-score of ≤−2.0. The diagnosis of osteoporosis in children was defined based on the 2019 International Society of Clinical Densitometry (ISCD) Official Positions as the presence of both a clinically significant fracture history (i.e., 2 or more long bone fractures by age 10 years or 3 or more long bone fractures by the age 19 years) and BMD Z-score ≤−2.0, or the finding of one or more vertebral compression fractures, regardless of BMD findings.[10]
3. Statistical analysis
Descriptive statistics, including mean, median, standard deviation and interquartile range (IQR), were used according to the normality of the data. Proportions or percentages were used to describe qualitative data. Independent samples t-test and Mann-Whitney U test were used for comparisons between 2 groups (low BMD vs. normal BMD, fractured vs. no fracture group). All statistical analyses were performed using Stata version 15.1 (StataCorp., College Station, TX, USA). A P-value less than 0.05 was considered to indicate statistical significance (2-tailed).
RESULTS
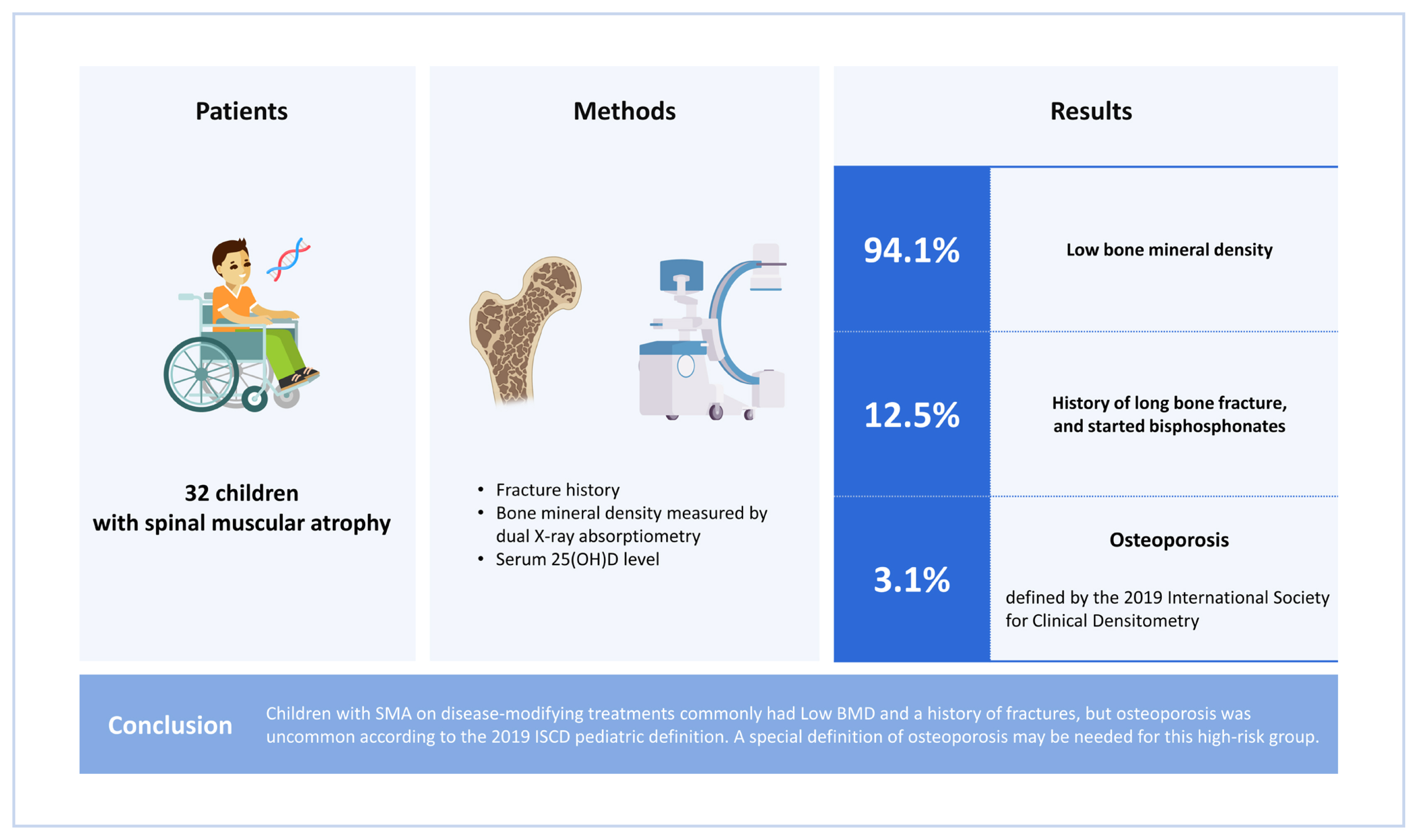
Thirty-two children were included (males, 12). Table 1 summarized their clinical characteristics. Eight had SMA type 1, 14 had SMA type 2 and 10 had SMA type 3. The median age was 10.8 years (IQR, 7.0-15.6 years). Twenty-six patients had been put on nusinersen for a median duration of 3.0 years (IQR, 2.0-4.0 years), while 7 patients had been on risdiplam for a median duration of 0.8 years (IQR, 0.7-0.9 years).
Thirty patients were taking vitamin D supplements (mean dose, 1,467±820 IU daily) and their mean 25-hydroxy-vitamin D (25[OH]D) level was 83.6±38.2 nmol/L. Only 3 patients had vitamin D insufficiency (range, 39-49 nmol/L).
BMD assessments by DXA were performed in 17 patients (All were on either nusinersen or risdiplam; nusinersen=11, risdiplam=1, nusinersen initially and changed to risdiplam later=3; SMA type 1=2, type 2=8, type 3=7). DXA was not performed in the remaining patients mainly because of significant fixed contractures hindering the positioning of scanning or parental refusal. When compared between the groups with or without DXA performed, there was no difference in age, sex, SMA types and ambulatory status.
The median BMD Z-score at TBLH was −5.0 (IQR, −5.5 to −3.5), LS was −2.1 (IQR, −2.7 to −0.4) and that at LDF R1, R2 and R3 were −3.2 (IQR, −4.0 to −2.9), −3.8 (IQR, −4.5 to −2.8) and −2.8 (IQR, −4.3 to −2.4) respectively (Table 2). Since all patients had a height Z-score of >−1, no height-adjustment on BMD Z-score was performed. A low BMD for age with Z-scores ≤−2 was observed in 16 out of the 17 patients with DXA performed. The only patient with a normal BMD for age had SMA type 3 with independent ambulation and was started on nusinersen 1.3 years ago. Only one patient fulfilled the 2019 ISCD definition of osteoporosis (3 episodes of long bone fracture by the age of 7 years).
Four SMA type 2 patients had a history of long bone fractures with trivial injury, e.g., during a change of diaper or physiotherapy (‘assisted sitter’=1, ‘sitter’=2, ‘assisted walker’=1). These patients were all put on bisphosphonates (zoledronic acid) when long bone fractures were healed. Bone turnover markers, including C-terminal telopeptide (CTX-I), N-terminal propeptide of type I collagen (P1NP) and alkaline phosphatase, were checked before the first bisphosphonate infusion when long bone fractures had been healed (patient 1 did not have the baseline CTX and P1NP measured due to inadequate blood sample collected), and they all had low or low normal bone turnover markers. All the 4 patients developed a high fever and 2 developed mild, asymptomatic hypocalcemia after the first infusion of bisphosphonates, but there were no other adverse effects in subsequent infusion (Table 3). The first patient also developed sputum retention after the first infusion, which was managed with vigorous chest physiotherapy. This patient had been given 8 infusions of zoledronic acid for 4 years with interval improvement in BMD Z-scores (Fig. 1). At the time of review, no further fractures have been observed among these patients after bisphosphonates treatment.
SMA types, age, sex, current state of ambulation, duration of disease-modifying treatment, and 25(OH)D level were not associated with fracture history or BMD Z-scores. In addition, BMD Z-scores were not associated with fracture history.
DISCUSSION
We described the bone health status of a group of children with SMA in Hong Kong. Like previous reports, low BMD for age and fractures were common among this group of children. However, only one fulfilled the 2019 ISCD pediatric definition of osteoporosis with low BMD for age (Z-scores ≤−2) and a clinically significant fracture history. Undoubtedly, the 2019 ISCD definition has successfully prevented overdiagnosis of osteoporosis and unnecessary treatment in healthy children who do not have true skeletal fragility. However, in the clinical context of children with immobility or exposure to osteotoxic medications, this definition could result in underdiagnosis, and subsequently, undertreatment of secondary osteoporosis. With the fact that even a single episode of long bone fracture could lead to permanent loss of ambulation, waiting for the second, even the third episode of long bone fracture would superfluously delay the initiation of treatment in these high-risk children. This raised the question of whether a special definition is needed for this high-risk group of children.
In the past, possibly related to the limited survival in patients with SMA, the issue of bone health was infrequently discussed. With the advent of disease-modifying treatments, which have enabled improved motor function, survival, and quality of life, there has been a paradigm shift in the overall care of children with SMA, with a greater focus on the associated comorbidities, including bone health. Indeed, fractures do not only lead to acute pain, but also potentially permanent loss of ambulation. Cast immobilization following fractures, especially if prolonged, could aggravate muscle wasting and bone loss and further speed up the disease progression. In the latest International Consensus of SMA care and management, importance of a multidisciplinary approach in the various aspects including bone health, has been highlighted, and regular bone health monitoring with annual DXA study and checking of 25(OH)D levels was recommended.[4] However, practical implementation in the real-world clinical setting could be challenging. In our cohort, only 17 out of 32 patients had a DXA study performed. The main reasons for not having a DXA study performed include difficulties in positioning due to contractures and parental refusal, as some do not prefer another hospital visit and are worried about the risk of additional investigatory procedures. Clearly, a better service model is needed to facilitate the delivery of this recommended multidisciplinary care.
When compared to other neuromuscular conditions like Duchenne muscular dystrophy (DMD), the bone health status of children with SMA is much under-reported. Table 4 summarises the published cohorts on the topic. The prevalence of low BMD, vitamin D deficiency and fractures observed in various cohorts varies, which is likely contributed by the heterogenous patients’ population with different SMA types motor functions across different studies, as well as different standards of care in terms of bone health monitoring.[2,3,11-14] This makes direct comparisons difficult. SMA types, phenotype severity, increasing age, motor function, serum 25(OH)D and parathyroid hormone level have been reported to be important factors influencing BMD in children with SMA.[2,3,14] We were not able to find any factors associated with low BMD or fracture, likely related to the small sample size of our study.
Unsurprisingly, in cohorts with larger sample sizes, children with SMA type 1 have been reported to have significantly lower BMD Z-scores at all skeletal sites than children with SMA type 2 or 3.[3] On one hand, muscle and bone function as one unit,[15] and hence it is to be expected that patients with more severe neurological phenotype would have weaker bones. On the other hand, the deficiency of SMN protein also has pronounced effects on BMD. In fact, it has been well described that children with SMA tend to have more severe reduction in BMD than in children with other neuromuscular conditions of similar level of mobility.[16] In mouse model, the SMN protein has been demonstrated to have important functional roles in skeletal development [17] and bone resorption activity by interacting with cellular signaling molecules such as osteoclast stimulatory factor 1 (OSTF1), which is involved in the indirect activation of osteoclasts.[18] Mouse models of human SMA were observed to have poorly developed caudal vertebra and pelvic bone fractures.[17] Abundant activated osteoclasts were also observed on the histochemical staining of vertebrae from SMA mice, consistent with increased bone resorption.[19] With a more severe SMA phenotype, the amount of SMN protein is also lower.[17,19] All in all, this accounts for the high prevalence of low BMDs and fractures among children with SMA, especially SMA type 1. Therefore, it is logical to deduce that, with disease-modifying treatment, the bone phenotype might also be modified and improved.
Previous studies have also shown that a significant proportion of children with SMA have high CTX levels, indicating higher bone resorption.[2,14] This could be explained by the functional roles of the SMN protein in bone resorption through the interaction with OSTF1.[18] However, this phenomenon was not observed in our 4 children with long bone fractures. Indeed, they all had low CTX and P1NP levels, indicating a low bone turnover state. This might reflect different extents of contribution of the SMN protein and immobility during different stages of the disease course.
Nasomyont et al. [20] described their experience in intravenous bisphosphonate therapy in 8 children with SMA. Similar to our experience, an acute initial reaction was common after the first infusion but not the subsequent infusions. Minimal acute adverse effects were observed, and the infusions were effective in reducing incidences of further fractures. However, an atypical femur fracture was observed in one patient, and hence caution is still needed.[20]
Interestingly, we observed a much higher mean LS Z-score than TBLH and LDF. This phenomenon was also observed in children with DMD.[21,22] This would be suggestive of more cortical bone defects than trabecular defects, as well as the differential weight-bearing effects on BMD at different skeletal sites — with some weight bearing at the spine but much less weight bearing at the lower limbs. Alternatively, it might also be attributed to the presence of artifacts induced by scoliosis, which is common among our children with SMA and may falsely increase the measured aBMD (Fig. 2). This highlights the complexity in DXA interpretation and limitations of aBMD assessment by DXA in this group of children. This also infers the need of exploring other novel imaging modalities e.g., peripheral quantitative computed tomography, as part of the bone health assessment.
Apart from long bone fractures, asymptomatic, undiagnosed vertebral fractures are indeed not uncommon and have been reported among young children with SMA at a prevalence of approximately 10%.[14] This underscores the importance of an annual vertebral fracture screening as part of the bone health assessment, which was not the standard of care in our practice before, but we have implemented this as our routine monitoring recently. In fact, with the recent commencement of service of the Hong Kong Children’s Hospital, a one-stop, multidisciplinary clinic with joint assessment by a pediatric neurologist, pediatric orthopedic surgeon, and pediatric endocrinologist has been set up since 2021. DXA scan is performed by dedicated radiographers experienced in handling children with medical complexities and fragile bones. In contrary to most centers DXA service is provided in the Radiology Department, we particularly designed the DXA service to be delivered in the ambulatory care center, which is just one floor above our clinic, with support from onsite pediatricians and nurses. All these arrangements would help reduce the anxiety of parents about the risk and inconvenience of additional investigatory procedures and facilitate better communication between different disciplines for comprehensive care delivery.
There are several limitations in this study. First, as a retrospective study, not all patients had undergone the bone health assessment with DXA. Patients’ diet history and calcium intake, as well as details on the skeletal geometry, were also not available, which could also contribute to their bone health status and fracture risk. The sample size was small. However, with limited publications on bone health status in this rare condition, this is still a valuable addition to the existing literature. It also provides further information on health service needs in this group of children for better planning of health care resources.
Low BMD and long bone fractures were common among children with SMA in Hong Kong but osteoporosis based on the 2019 ISCD definition was uncommon. This latest ISCD pediatric definition of osteoporosis may result in underdiagnosis in this group of at-risk children and could potentially delay appropriate treatment for osteoporosis. Despite clear recommendations on regular bone health surveillance, practical implementation in the real-world could be challenging. Modifications in the care delivery system, e.g., a one-stop multidisciplinary service model, would facilitate the practical implementation. Longer-term, prospective studies with larger sample sizes are needed to investigate the effect of disease-modifying treatment and bisphosphonates on skeletal phenotypes in this group of children.


 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Print
Print






