



INTRODUCTION
Secondary fracture preventions (fracture liaison service [FLS]) including anti-osteoporotic medication and patient education are important for fragility fractured patients because of the high rates of re-fracture after the first fracture [1]. Among fragility fractures including spine, hip, wrist, and proximal humerus, hip fractures are notorious to high mortality, morbidity, and a socioeconomic burden in an aging society. According to recent studies, numbers of fragility fractures are expected to increase trends in the future [2,3]. Secondary fracture prevention programs can be configured in a variety of forms depending on the country's medical system and hospital capacity, and are currently operating in 35 countries around the world [4]. Reported secondary fracture prevention programs can be divided into two main categories. The first is to report the clinical outcomes such as changes in the rate of evaluation and management of osteoporosis or changes in the re-fracture rate after the second fracture prevention program [3,5-7]. The second is proven the economic effect of the second fracture prevention program [8]. Those programs have the same purpose of operation but vary in the way they operate and their members.
Although the management of the secondary fracture prevention program is performed in various ways, the coordinator is important for multidisciplinary management [2]. The role of the coordinator is considering assessment of the past medical history of patients, arrangement of the necessary examinations for osteoporosis, engagement in communication with the primary physician after discharge, and communication among the medical staff in the hospital. They can also help patients to understand the need for osteoporosis evaluation and anti-osteoporotic medication use and to maintain the continuity of patient care. However, there are only a few reports of what role coordinators perform in these secondary fracture prevention programs, and there is no globally recognized training program for them. The hypothesis of this study is that the role and assignment of the coordinator will vary among FLS studies.
Therefore, the purpose of this study is to search for reports on the clinical effectiveness of FLS being implemented worldwide through the systematic review, analyze the roles of coordinators in each study, and provide basic data for the development of future coordinator education programs.
METHODS
A systematic search of the literature using the Medline, PubMed, and EMBASE databases and the Cochrane Library was conducted for publications (January 2000-October 2019 inclusive) using the following keywords: ‘osteoporosis’ AND ‘fractures’ AND ‘secondary prevention’. The detailed search method is shown in the Supplementary Appendix 1. Relevant papers have also been searched for other local repositories, blogs, and gray literature outlets. The systematic reviews adhere to the Cochrane Collaboration approach.
Inclusion criteria for the trials were: performed in patients ≥50 years of age with all forms of osteoporosis-related fractures; randomized or non-randomized stage 1 to 4 studies; retrospective or prospective observational studies. Excluded are research relating to the prevention of primary fractures or other bone-associated diseases, forms of narrative analyses, systematic reviews, meta-analysis, opinion articles, editorials, case reports, letters, and publications in languages other than English. Two independent reviewers selected the studies by first screening the title and abstract followed by full-text articles. The discrepancy between the 2 reviewers was resolved by consensus or by a third independent reviewer, if necessary. Data analysis used the parameters Population, Procedure, Contrast, Outcomes, Environment (PICOS) and included general information about the article (e.g., authors, publication year), study characteristics (e.g., design, sample size), patient characteristics (e.g., fracture type, osteoporosis duration), and outcomes (bone mineral density testing, treatment initiation, adherence, persistence, rates of re-fracture, and mortality).
Data synthesis and findings were reported in the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) statement. Quality assessments of eligible study methodologies were conducted using the Newcastle - Ottawa scale for non-randomized studies. These 2 authors independently assessed the quality of all studies.
RESULTS
1. Searched Studies of FLS in Various Countries
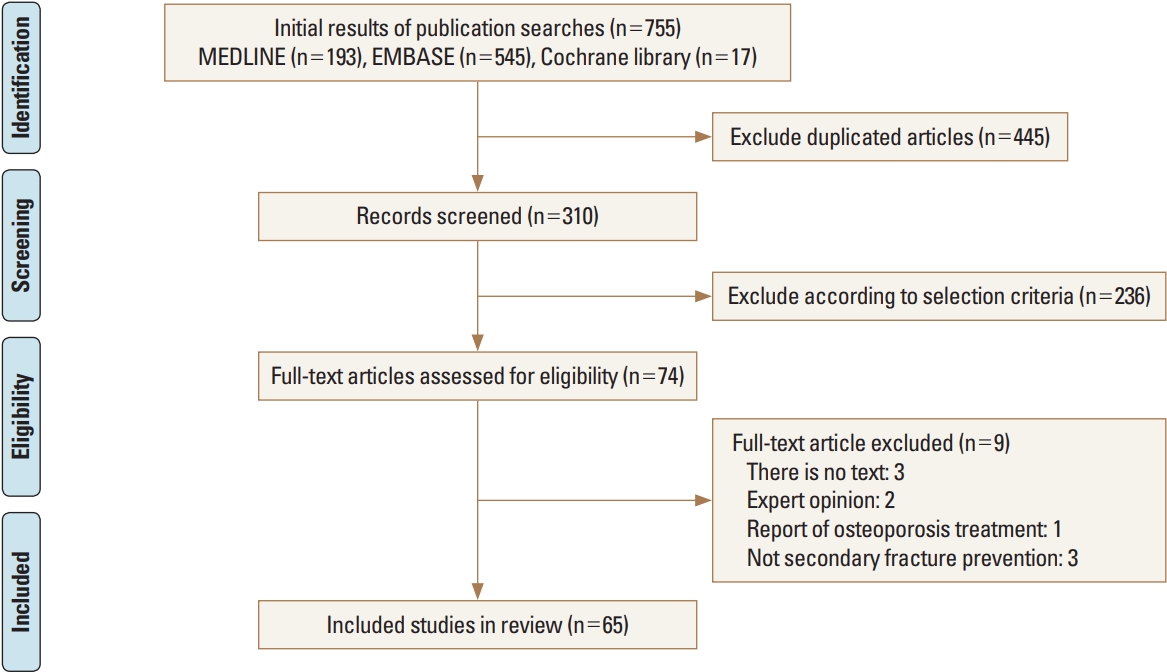
The initial search identified 755 references from the selected databases. The 681 references were excluded by screening the abstracts and titles for duplicates, unrelated articles, case reports, systematic reviews, and non-comparative studies. The remaining 74 studies underwent full-text reviews, and subsequently, nine studies were excluded. Finally, 65 studies are included in this study. The details of the identification of relevant studies are shown in the flow chart of the study selection process (Fig. 1). Seventeen randomized controlled studies, 26 comparative studies, and 22 cohort observation studies were selected for further investigation [1-3,5-7,9-66]. The main characteristics and outcomes of the studies included in this systematic review are presented in Table 1.
Reported studies for second fracture prevention programs were performed in the USA, Canada, and Australia et al. from 2002 to 2017. The most common type of fracture in included studies was hip (57 studies), followed by wrist (43 studies) and humerus (38 studies) fracture.
The most used name of the program was FLS in 18 studies (Table 2). There were also 16 programs containing “intervention”. There were 9 studies involving the expression "integrated" or "multidisciplinary" or "multifaceted". There were also 5 studies that included the expression "fracture prevention" or "secondary prevention".
2. Naming and Roles of Coordinators in FLS
Coordinator is mentioned in various ways in each study (Table 2). Expression including “nurse” is observed in 20 studies and 11 studies include “coordinator”. In the 6 studies, they were called “manager”, and there were 26 studies that did not mention them. Three studies have also mentioned their real names directly.
There were 31 studies describing the role of the coordinator directly, but 34 studies did not describe the role of the coordinator directly. The described roles of coordinator in included studies can be categorized into 9 roles (Table 3). The most common description is “explaining to the patient the need for osteoporosis evaluation and management” and “identifying the patients to be included in the secondary fracture prevention program” was described in 18 studies. “Casual link with patients” and “patient assessment” are also described as coordinator roles.
3. Results of Quality Assessment
The quality assessment for retrospective observational comparison studies using the modified Newcastle-Ottawa Score Tool is measured. All of the included studies were described as observational studies. Sample size calculations were not performed in all studies. The representation of the selected samples was considered appropriate in all included studies. The ascertainment of the assessment tool for sarcopenia was considered as adequate in all observational studies. The response rate, consideration of important confounding factors, ascertainment of assessment tool, and statistical evaluation were reported in all studies. Overall, all of the included individual studies were considered to have a low risk of bias.
DISCUSSION
In this systematic review, the program of FLS was found to be reported in various forms. There was a model in which patients were screened by pharmacists and evaluated for osteoporosis while a consultation program was provided to the hospitalist or rheumatologist for evaluation and treatment of osteoporosis [20,35,67]. There was also an electronic medical record reminder to increase osteoporosis management in fragility fracture patients [23]. Most of the patients with fractures under the program were older than 50 years of age, but there were programs with inclusion of lower age limits of 40 or 45 years old, and one study had no age limitation [33,51,61,65].
At the coordinator-based FLS center, the coordinator (often a nurse) acts as a central player in the establishing of patient connections, orthopedic surgeons, radiologists, and attending physicians. Coordinators help bridge the nursing gap by supporting identification, investigation, initiation of treatment, and patient follow-up. Medics has opened the way to effectively manage patients at high risk of developing another fracture. In addition, nurses are in a unique and important role as nurses responsible for enhancing their daily lives by building relationships with patients and families.
Based on the results of this systematic review, the role of the FLS coordinator are summarized by explaining the need for osteoporosis evaluation and management, promoting follow-up with primary physicians, recognizing patients, collecting data, evaluating patients, obtaining research approval, casual or daily follow-up, consulting with physicians or transferring information to physicians, coordinating the test. Yuksel et al. [67] reported that osteoporosis assessment was increased, but there were many patients who did not receive appropriate care. For this reason, the authors of these studies attempted to explain the lack of knowledge of the patient and general practitioner, a lack of awareness of current treatment guidelines by both family physicians and orthopedic surgeons, and a perception by orthopedic surgeons. practitioners, poor compliance with prescribed medications and a general lack of communication between all health care providers involved in managing a patient with a fragility fracture. There is a lack of understanding and communication between the patient and the medical staff about this condition, and continuous management of the patient is needed, and this can be done by the coordinator. So, as the results of our study, the most commonly mentioned and important role of the coordinator may be explaining the need for osteoporosis evaluation and management to patients and their families.
Mentions of Coordinator training were observed in 6 studies [17,34,42,44,59,66]. A study by Gardner et al. [42] mentioned that coordinators trained regarding the discussion of the role of osteoporosis in hip fractures, the importance of preventing future fractures, and the effectiveness of currently available therapies. Majumdar et al. [55] stated that the experienced nurse had additional training and expertise in the diagnosis and treatment of osteoporosis. Huntjens et al. [34] described that fracture nurse trained in osteoporosis management and fall risk-assessment [17,34, 42,44]. Mentioned only trained nurses and did not give specific details [59,66].
Although the exact career is not described in many studies, the most commonly mentioned career is a nurse. In terms of medical experience, a nurse may be very suitable for the coordinator and may not require much additional training. Depending on the names of specialist nurses, rheumatology nurse managers, orthopedic nurses, and fracture liaison nurses, you can estimate the major department of nurse affiliation or program operation [22,25,52,58].
In the included studies, the types of fractures for the prevention program also varied. In the study of Kuo et al. [64], all minimal trauma fractures were included, but fractures of finger, toe, and skull were excluded. The subjects of Eekman et al. [46] were similar to that of Kuo’s study, but were excluded facial bone fractures. Because the study of Collinge et al. [51] covers all fracture patients over the age of 18, all fractures in addition to low energy trauma were included in the study. Surely, hip was the most frequently mentioned fracture sites managed by the FLS program. In some studies, vertebral fractures were excluded because they did not increase mortality [5,34]. Hurrington and Lease [50] and Beaton et al. [2] included pelvic fractures in the subjects.
This study has several limitations. First, only limited information could be extracted from these selected papers. Although included studies have reported the role of the FLS coordinator, most studies do not mention detailed protocols of an education program for FLS coordinator. Therefore, it is important to share information on the role of FLS coordinator, and actual educational programs of the FLS coordinator through consensus meetings and academic meeting on different continents. Second, we only included papers that were found after a systematic search against scientific databases. Thus, grey literature on this topic, including abstracts of presentations at meetings on FLS, was not included in this systematic review. Third, we have included retrospective studies, and it may make some biases for data analysis. But, we didn’t perform statistical analysis and just collected for the descriptions of the role of coordination in FLS. Thus, we believe that there are a few possibility for risk of bias by including retrospective studies in our study.
The importance of FLS has been proven in many studies. In addition, it is also reasonable to say that the coordinator is a member who plays a key role in the successful progress of the fracture prevention program between doctors and patients. However, it seems showed that the roles of coordinators and educational programs were not unified worldwide. In our best knowledge, this is the first study for analysis about the roles of coordinator and their education. Based on the results of this study, it is considered that the role of the coordinator should be clearly defined, and efforts should be made to activate the educational program for coordinator training.
CONCLUSIONS
In conclusion, the coordinator in the FLS program plays an important role in multidisciplinary management of vulnerable fractures, as well as in the diagnosis and treatment of osteoporosis and in maintaining continuity of treatment. In the future, the broader role of coordinators should be systematically organized and developed into accredited educational programs.
 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Full text via PMC
Full text via PMC Download Citation
Download Citation Supplement
Supplement Print
Print






