Analysis of Clinical Features of Hip Fracture Patients with or without Prior Osteoporotic Spinal Compression Fractures
Article information
Abstract
Background
To analyze and compare the clinical characteristics including bone mineral density (BMD) in a group who had operation of hip fracture with or without prior osteoporotic spinal compression fractures.
Methods
Two hundred forty patients who had undergone operation of hip fractures were evaluated, 127 patients who had with prior osteoporotic spinal compression fractures were in group I, and 113 patients without prior spinal fractures were in group II. In each group, we measured age, gender, body mass index (BMI, kg/m2), BMD (mg/cm3), type of hip fractures, concomitant diseases, presence of secondary hip fracture and history of percutaneous vertebroplasty.
Results
The mean age of group I was 79.4 years (male/female: 28/99) and that of group II was 77.6 years (male/female: 37/76). The mean BMI of group I was 21.3 kg/m2 and that in group II was 22.0 kg/m2. The mean BMD and T-score of group I were 41.1 mg/cm3 and -4.45 and those in group II were 51.0 mg/cm3 and -4.17 (P<0.05). The numbers of patients of neck and intertrochanter fracture of group I were 31 and 96 patients and those in group II were 61 and 52 patients. Sixty in group I and 45 in group II patients had concomitant diseases. Thirteen patients had undergone percutaneous vertebroplasty and 18 patients (7.5%) had second hip fractures.
Conclusions
The hip fracture patients who had with prior osteoporotic spinal compression fractures had lower BMD compared to the hip fracture patients without previous spinal compression fractures.
INTRODUCTION
Recent studies reported increasing risks of hip, spine, and others among people who had previous clinically diagnosed fractures, or radiographic evidence of vertebral fractures.[1,2] Also, spinal radiographs identifying of prevalent vertebral deformities may be useful additional measurement to classify further a women's risk of future fracture.[1] Women with preexisting vertebral fractures had approximately 4 times higher risk of subsequent vertebral fractures and 2.3 times greater risk of subsequent hip fractures than those without prior fractures.[2]
Percutaneous vertebroplasty is one of the most commonly performed procedures for symptomatic osteoporotic spinal fractures.[3,4] But, subsequent fracture of spine is a potential complication of vertebroplasty.[3,5] There are many reports of subsequent vertebral fracture while there are only a few reports of non-vertebral fracture, especially, hip fractures after percutanous vertebroplasty in osteoporotic spinal compression fracture. This present study aim to analyze and compare the clinical characteristics of bone mineral density (BMD) in a group of hip fracture patients whether or not prior osteoporotic spinal compression fractures by cohort retrospective study. Additionally, whether or not of secondary hip fracture and history of percutaneous vertebroplasty in both groups were investigated.
METHODS
We reviewed 240 patients over 65 years of age among 436 cases who had undergone operation of intertrochanteric and neck of hip fractures in one hospital by retrospective study from June 2006 to June 2012. We excluded patients who had hip fracture by high velocity injury such as a motor vehicle accident or falling down from height, those with under 65 years of age, unexamined BMD, and previous spine fusion operation. We checked BMD and simple thoracolumbar radiograph of whole patients at the time of injury. The patients were divided into prior osteoporotic spinal compression fractures in group I (127 patients, male/female: 28/99) and without compression fractures in group II (113 patients, male/female: 37/76). In each group, we measured age and gender, body mass index (BMI, kg/m2) with weight and height, type of hip fractures, concomitant diseases, and presence of secondary hip fracture and undergone percutaneous vertebroplasty. The fractures were classified as hip fractures in intertrochanteric and femoral neck fractures. The definition of second hip fracture was patients who have suffered a hip fracture with a subsequent fracture of the contralateral hip. The included concomitant diseases were hypertension, diabetes mellitus, cardiac disease, and senile dementia.
Assessment of prior radiographic vertebral fractures has been by a radiologist and two orthopedic surgeons. Six points digitations on each vertebral body of the thoracic and lumbar lateral radiograph for quantitative morphometry were done as described previously, so that the anterior, middle, and posterior heights could be accurately measured.[6,7] Baseline prevalent deformities were defined using a modified Melton/Eastell vertebral height ratio criteria.[6] BMD was measured utilizing peripheral-quantitative computed tomography (P-QCT; Somatom sensation 16, Simens, Erlangen, Germany) of thoracolumbar vertebrae that enables separate analyses of cortical, trabecular and total bone density including T-score.
Quantitative variables (age, BMI, BMD and T-score) were compared between groups by an independent T-test and difference in the categorical variables (sex, hip fracture type and concomitant disease) were compared using the chi-square test. The Mann-Whitney U test for continuous variables was used. SPSS version 20.0 (SPSS Inc., Chicago, IL, USA) was used for the statistical analyses. A P value of less than 0.05 was considered statistically significant.
RESULTS
The mean age of group I was 79.4 years (range, 65 to 95 years) and group II was 77.6 years (range, 65 to 93 years). The mean BMI of group I was 21.32±4.2 kg/m2 (mean weight/mean height: 51.8 kg/155.9 cm) and group II was 22.03±3.4 kg/m2 (mean weight/mean height: 55.9 kg/158.9 cm). The mean BMD and T-score of group I were 41.12±21.9mg/cm3 and -4.45±0.8 and those in group II were 51.00±20.3 mg/cm3 and -4.17±0.7. The age of group I was relatively older than those of group II (P=0.124), but the BMIs had no significant difference between groups (P=0.293). The BMD of group I was significantly lower than those of group II (P<0.001). Also, the T-score of group I was significantly lower than those of group II (P=0.007) (Table 1). The numbers of patient of neck and intertrochanter fracture of group I were 31 (24.4%) and 96 (75.6%) patients and those in group II were 61 (54.0%) and 52 (46.0%) patients, retrospectively, which have a statistical significance (P<0.001). Twenty-four patients (64.9%) among 37 male patients in group II had the type of neck fracture. Sixty (47.2%) in group I and 45 (39.8%) in group II patients had concomitant diseases, hypertension was the most common concomitant disease 46 in group I and 34 in group II patients.
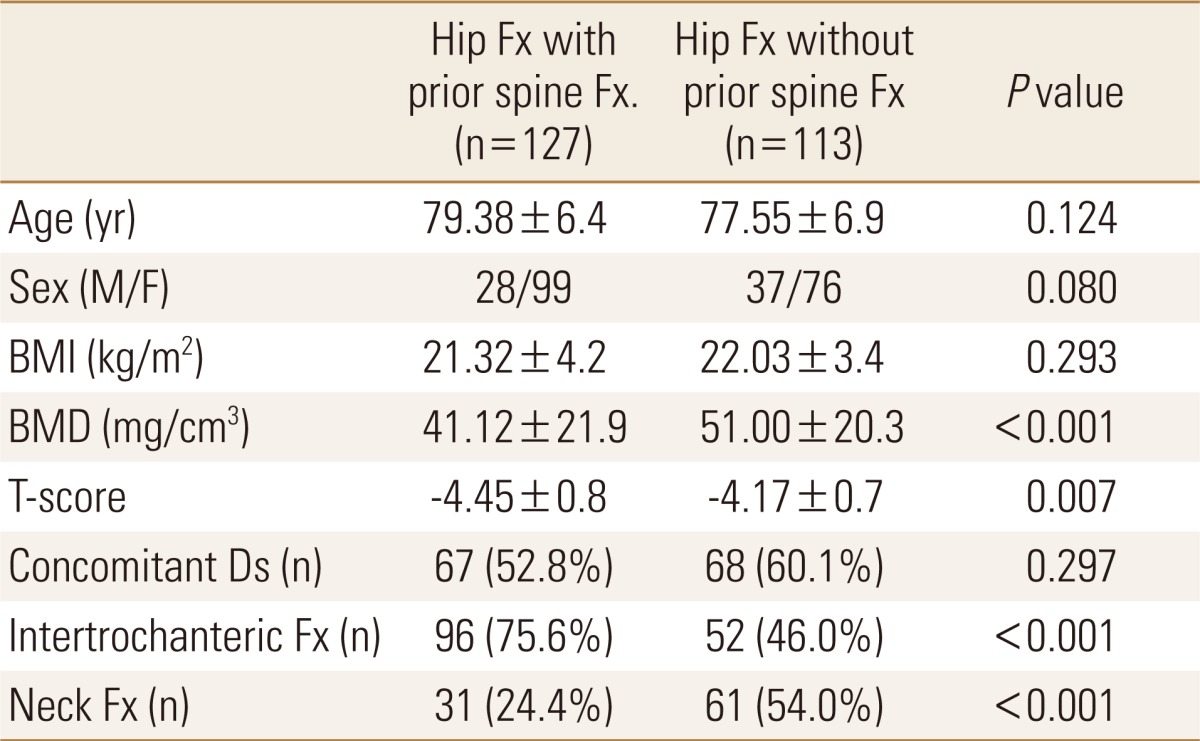
Demographic data
Only 13 patients (5.4%) among 240 patients had undergone percutaneous vertebroplasty (males/females: 2/11) and the mean age was 78.5 years (Table 2). Twelve in group I and six in group II patients had operation due to second hip fracture and the mean age of them was 82.7 years (males/females: 6/12). The age of patients of second hip fracture was significantly older than those of unilateral hip fracture patients (P=0.006) (Table 3).
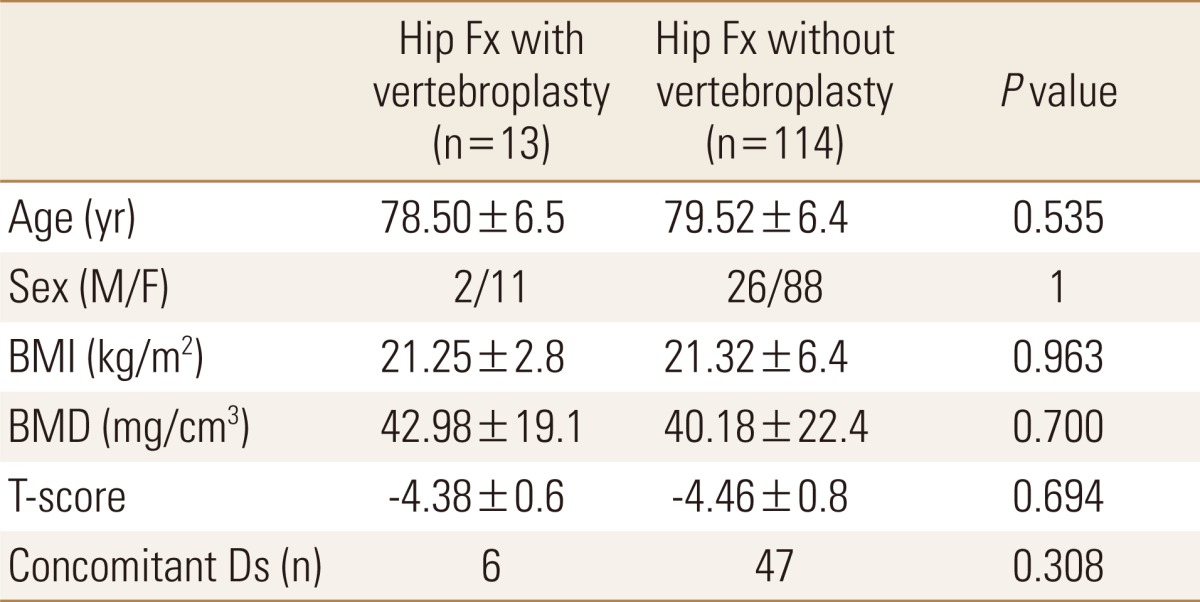
Comparison of between hip fracture with or without vertebroplasty
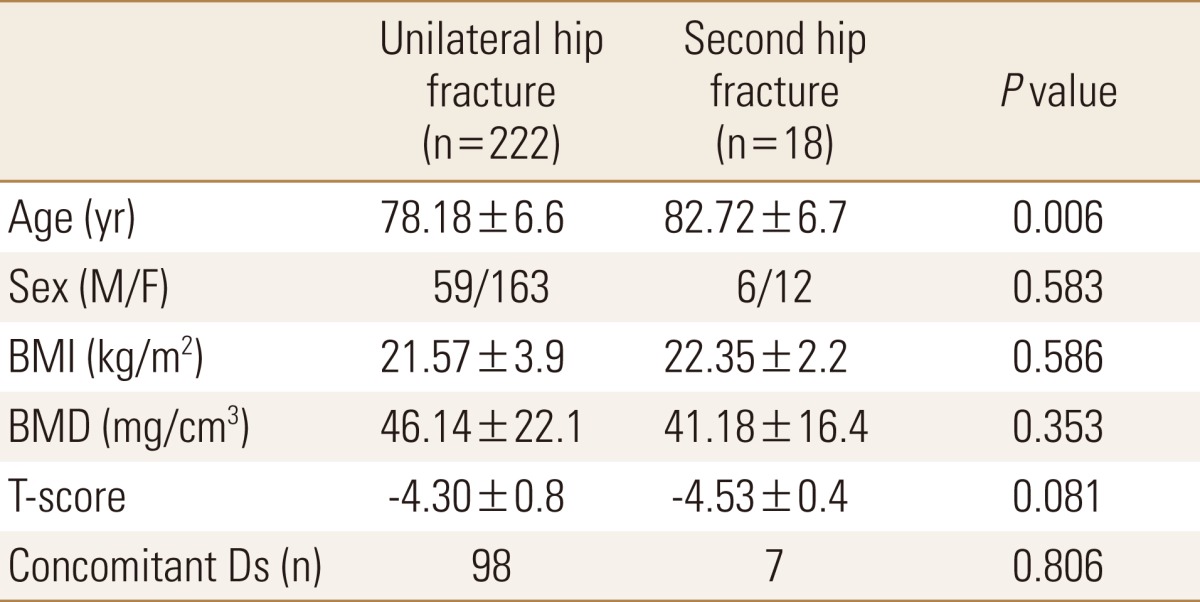
Comparison of between unilateral hip fracture and second hip fracture
DISCUSSION
The incidence of osteoporotic fracture is rising due to increasing of people living to an older age. Prior fractures have been documented consistently to predict the risk of subsequent incident fractures.[1,2,7] Many studies had demonstrated that prevalent vertebral fractures are risk factors for incident hip fracture and that predicts future vertebral and hip fractures.[1,7-9] In large meta-analyses, the pooled estimates for the risk of a subsequent hip fracture were found to be approximately twofold in the presence of vertebral fracture.[2,10] However, only a few reports discussed about non-vertebral fracture, especially, hip fractures after percutanous vertebroplasty in osteoporotic spinal compression fracture. Mazzantini et al.[11] reported in patients with osteoporosis treated with pecutaneous vertebroplasty, the incidence of new vertebral fractures was 27.8% and non-vertebral fractures occurred in only 7% (only one at the hip) in as few as 3.5% of the patients if exclude rib fractures after 39 months. In our study, only 13 patients (5.4%) had undergone percutaneous vertebroplasty in 240 patients who had undergone operation of hip fractures, retrospectively. The incidence of second hip fracture has been reported to be about 5% -10% and is expected to increase with the aging of the population in the future.[12,13] It has previously been reported that age and female sex are important risk factor for hip fracture.[14,15] However, some reports have indicated that there are no differences in age or sex between unilateral and second hip fractures.[12,16] Mitani et al.[12] reported that the mean age at the time of initial fracture in the second fracture group tended to be slightly older than the mean age of the unilateral group. In our study, 18 patients (7.5%) had operated of second hip fractures in mean age 82.7 years. The age of patients of second hip fracture was significant older than those of unilateral hip fracture patients. Female patients were 12, and male patients were 6 among 18 patients of second hip fracture.
Bone strength has been described as a reflection of the integration of bone density and bone quality.[17] BMD is strongly associated with fracture risk. Therefore, an important clinical goal is to prevent the bone loss that leads to the first fracture, because this bone loss is largely irreversible by the time the first fracture occur. Across the range of BMD T-score, spine fracture burden had up to a 12-fold impact on the predicted vertebral fracture risk but only approximately twofold impact on predict non-vertebral fracture risk.[2] Siris et al.[8] stated that at any given BMD T-score, the risk of incident vertebral, non-vertebral, and any fracture depended heavily on prevalent radiographic vertebral fracture status. Most women with a history of low trauma risk fractures have low BMD, and women with both low BMD and prior fractures had a very high risk of further fractures. In our study, the BMD and T-score of multiple fractures group was significant lower than hip fractures group.
Our study has limitations of a relatively small number of patients. The main reason for small number was the rate of diagnosis osteoporosis of the hip fracture patients in early period (2006-2009: 51.5%) less than in late period (2010-2012: 82.5%) of our study period. Many studies have reported low rates of osteoporosis treatment after hip fracture.[18,19] This result suggests that the orthopedic surgeon can perform a leading role in the prevention of further fractures. We agree that the orthopedic surgeons can serve a pivotal role in optimizing treatment, not only of the fracture, but also of the underlying disease.[20] Second, we only considered operated hip fracture patients with or without prior osteoporotic spinal compression fractures by retrospective study, but the long term prospective study of patients treated with percutaneous vertebraoplasty is needed.
In summary, the hip fracture patients who had with prior osteoporotic spinal compression fractures had lower BMD and T-score compared to the hip fracture patients without previous spinal compression fractures. These multiple osteoporotic fracture patients should be clinically evaluated and treatment for osteoporosis.
Notes
This paper was supported by Wonkwang University in 2013.
No potential conflict of interest relevant to this article was reported.