Prevalence of Sarcopenia Adjusted Body Mass Index in the Korean Woman Based on the Korean National Health and Nutritional Examination Surveys
Article information
Abstract
Background
The purpose of this study was to determine cut-off point of appendicular skeletal muscle mass (ASM) adjusted body mass index (BMI) for sarcopenia in the Korean women and evaluate the prevalence of sarcopenia in postmenopausal women.
Methods
This study was based on the data obtained from 2008 to 2011 Korean National Health and Nutrition Examination Survey (KNHANES) IV and V. A whole body dual energy X-ray absorptiometry (DXA) scan and measurement of BMI were performed on individuals of ≥10 years old. Five thousand, two hundred and fifteen women older than 50 years were included in the study. ASM was obtained by adding the muscle masses of the four limbs. To determine the young reference group, mean and standard deviation of ASM and ASM/BMI by ages was measured. We calculated the prevalence rate of sarcopenia by each age group according to the cut-off point based on ASM and ASM/BMI.
Results
In determining the cut-off values related ASM/BMI, using the value that is two standard deviations below mean values for young reference group (20's and 30's) thus recommends 0.50 m2 in women. The overall prevalence among women older than 50 years was 15.6%. Among women older than 65 years prevalence of sarcopenia was 22.9%.
Conclusions
The prevalence of sarcopenia among Korean women obtained in this study is within the proper range of value to research about sarcopenia. Furthermore, using 0.50 m2 as the cut-off value can help compare various studies about sarcopenia in Korea.
INTRODUCTION
Sarcopenia will have its own International Classification of Disease, in the Tenth Revision, Clinical Modification (ICD-10-CM). The assigned code will be M62.84 and it will be available for use as of October 1, 2016.[1] In spite of this clinical importance of sarcopenia in the elderly, the criteria for its definition and clinical diagnosis are not yet clear-cut and vary among studies and experts.[23]
For this reason, several groups of experts have convened recently to establish consensus diagnostic criteria for sarcopenia.[456] Although the criteria lacks clinical evidence, this is a significant advance since many studies can now be conducted based on a single criteria without confusion. Asian Working Group for Sarcopenia (AWGS), which includes Korea, is also one of the efforts.[6] Korea is one of the most rapidly aging countries and a number of studies focusing on the prevalence, etiology, and clinical issues of sarcopenia have been released recently in Korea. However the criteria for the definition of sarcopenia vary among different studies. Furthermore, since the distribution of the muscle mass and heights of Korean women in each age group differs from that of other countries, there were even more confusions in defining the cut-off values.
One of the biggest problems in sarcopenia research on Korean elderly, especially in women, is that the younger generation is taller than older generation and has lower height-adjusted muscle mass (appendicular skeletal muscle mass [ASM]/height2 [Ht2], ASMHt2).[7] As a result, the prevalence of sarcopenia differed markedly among studies using.
Recently, the new diagnostic criteria of sarcopenia adjusting body mass index (BMI) was introduced by the Foundation for the National Institutes of Health (FNIH) sarcopenia project in 2014.[8] However, there is a concern over which group will be the young reference and which value will be the cut-off point. Therefore, the purpose of this study was to determine cut-off point of ASM adjusted BMI for sarcopenia in the Korean women and evaluate the prevalence of sarcopenia in postmenopausal women.
METHODS
This study was based on the data obtained from 2008 to 2011 Korean National Health and Nutrition Examination Survey (KNHANES) IV and V, a nationally-representative survey conducted by the Korean Ministry of Health and Welfare. A whole body dual energy X-ray absorptiometry (DXA) scan and measurement of BMI were performed on individuals of ≥10 years old from July 2008 to May 2011. Five thousand, two hundred and fifteen women older than 50 years were included in the study. Written informed consent was given by all participants and the protocol for KNHANES IV and V were approved by the Institutional Review Board of the Korean Center for Disease Control and Prevention (KCDC).
In the KNHANES study, whole body DXA examinations were conducted with a QDR4500A apparatus (Hologic Inc., Bedford, MA, USA). The data includes values for bone mineral content (g), bone mineral density (g/cm2), fat mass (g), lean mass (including bone mineral content [g]), and fat percentage of whole body and anatomical regions. From this data, ASM was obtained by adding the muscle masses of the four limbs, which were calculated by assuming that all non-fat and non-bone mass is skeletal muscle.
To determine the young reference group, mean and standard deviation of ASM and ASM/BMI by ages was measured. In the distribution of ASM and ASM/BMI, we selected 20-year which is a peak for each age group and recommended two standard deviations below mean values for young reference group as the cut-off point. Also, we calculated the prevalence rate of sarcopenia by each age group according to the cut-off point based on ASM and ASM/BMI.
1. Definition of terminology
1) Elderly
Elderly person is defined as 65 years and over in our study. The status of society is divided into three categories based on proportion of population of 65 years and over: Ageing society (7%-14% elderly population), aged society (14%-20%), super-aged society (exceed 20%).[910]
2) Postmenopause
According to Gallup survey 2001, Korean women undergo menopause at 49.7 years on average. Therefore, women older than 50 years are potentially regarded as postmenopausal in this study.
3) Geripause
Geripausal women is defined if she is 65 years or over. Early geripausal women is 65 to 85 years and late geripausal women is aged 85 years and over.[11]
4) Statistical analysis
Age-groups were divided into 9 groups (10's, 20's, 30's, 40's, 50's, 60's, 70's, 80's, and 90's) and described demographic trend of ASM mass, ASM/BMI of each age groups. We calculated the mean ASM and ASM/BMI of young reference of each age group and calculated incidence of sarcopenia in women. All analyses were conducted using SPSS software version 20.0 (SPSS Inc., Chicago, IL, USA).
RESULTS
KNHANES that was performed from 2008 to 2011 involves 11,621 women aged 10 to 97 years. Mean and standard deviation of year was 46.73±18.54 years. Age distribution was 1,012 (8.7%) in 10's, 1,236 (10.6%) in 20's, 2,098 (18.1%) in 30's, 2,065 (17.8%) in 40's, 1,965 (16.9%) in 50's, 1,714 (14.7%) in 60's, 1,236 (10.6%) in 70's, 284 (2.4%) in 80's, 11 (0.1%) in 90's (Table 1). The characteristics of subjects by ages are detailed in Table 1.

Distribution of appendicular skeletal muscle mass (kg) and appendicular skeletal muscle mass/body mass index (m2) by ages
1. Changes of ASM mass and ASM/BMI
The mean ASM was progressively increased from 10's to 40's: 13.53 kg in 10's, 14.72 kg in 20's, 14.80 kg in 30's, 14.87 kg in 40's. After which the mean ASM was progressively decreased till 90's: 14.53 kg in 50's, 14.17 kg in 60's, 13.28 kg in 70's, 12.38 kg in 80's, 11.47 kg in 90's. Two groups that have peak mean ASM were 30's and 40's (Fig. 1A).
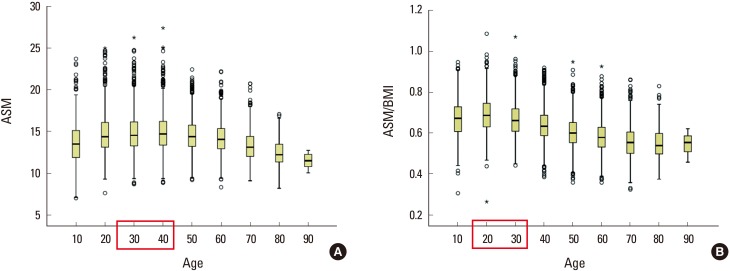
(A) Distribution of appendicular skeletal muscle mass (ASM; kg) by ages. (B) Distribution of ASM/body mass index (BMI; m2) by ages.
The mean ASM/BMI was progressively increased from 10's to 20's: 0.67 m2 in 10's, 0.70 m2 in 20's. After which the mean ASM/BMI was progressively decreased till 90's: 0.67 m2 in 30's, 0.64 m2 in 40's, 0.60 m2 in 50's, 0.58 m2 in 60's, 0.56 m2 in 70's, 0.55 m2 in 80's, 0.55 m2 in 90's. Two groups that have peak mean ASM were 20's and 30's (Fig. 1B).
2. Calculation of Korean cut-off value by different references
In determining the cut-off values related ASM and ASM/BMI, using the value that is two standard deviations below mean values for young reference group (30's and 40's) and (20's and 30's) thus recommends 0.49 m2 (mean±SD, 0.65±0.08 m2) and 0.50 m2 (mean±SD, 0.68±0.09 m2) in women, respectively. We used 0.49 m2 and 0.50 m2 as the cut-off values to identify prevalence for sarcopenia among women in Korea, respectively.
3. Prevalence of sarcopenia in postmenopausal and geripausal women by different cut-off values
Prevalence of sarcopenia using cut-off value of 0.49 m2 was 122 (6.2%) in the 50's, 172 (10.0%) in the 60's, 263 (21.3%) in the 70's, 66 (23.2%) in the 80's and 3 (27.3%) in the 90's (Table 2). The overall prevalence among women older than 50 years was 12.0%. Prevalence of sarcopenia using cut-off value of 0.50 m2 was 165 (8.4%) in the 50's, 240 (14.0%) in the 60's, 323 (26.1%) in the 70's, 81 (28.5%) in the 80's and 3 (27.3%) in the 90's (Table 3). The overall prevalence among women older than 50 years was 15.6%.
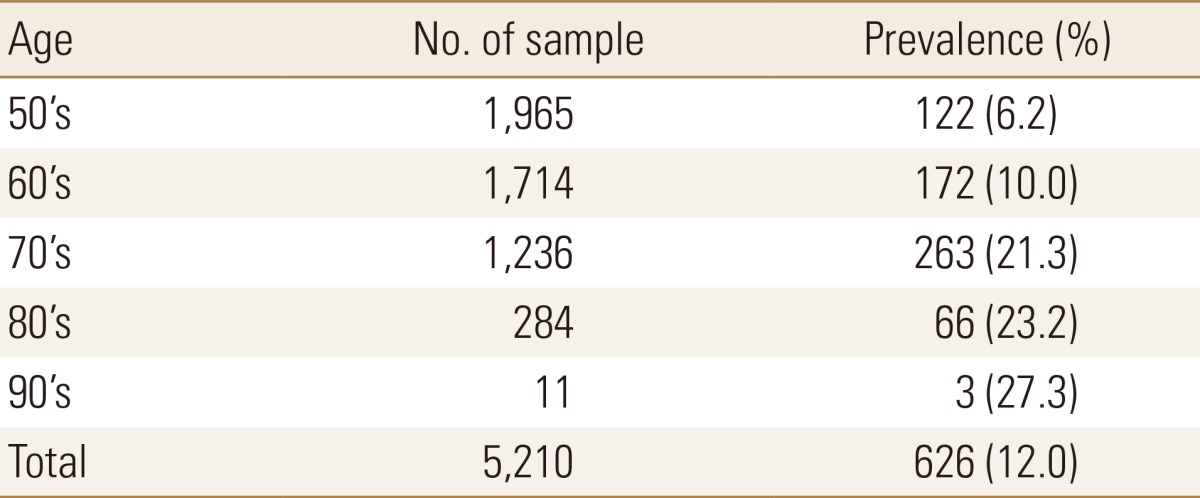
Prevalence (%) of sarcopenia using cut-off of 0.49 m2 in postmenopausal women
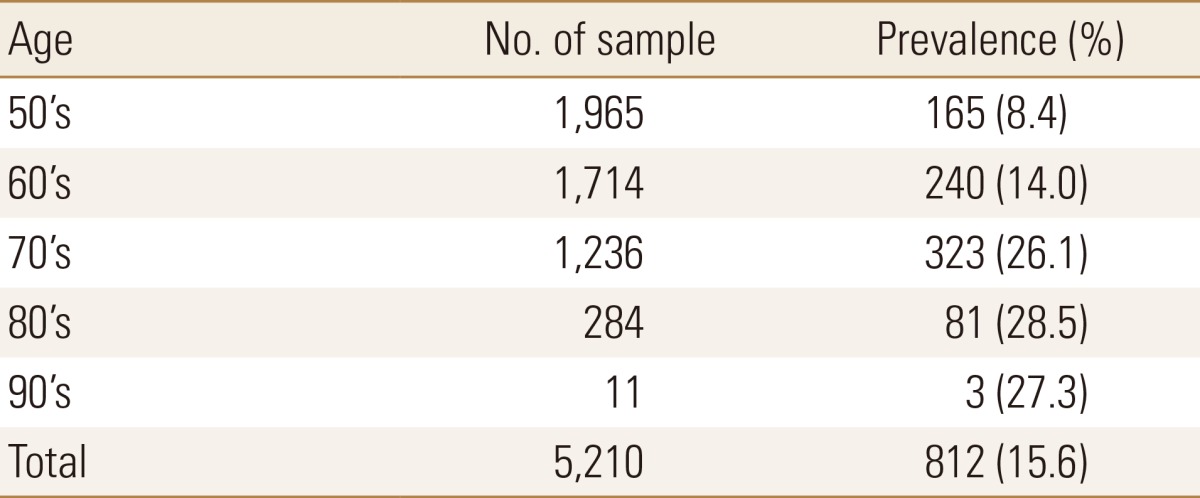
Prevalence (%) of sarcopenia using cut-off of 0.50 m2 in postmenopausal women
Prevalence of sarcopenia using cut-off value of 0.49 m2 was 233 (14.5%) at aged 65 to 74 years, 165 (23.4%) at aged 75 to 84 years, 19 (24.1%) in more than 85 years. Among women older than 65 years prevalence of sarcopenia was 17.4% (Table 4). Prevalence of sarcopenia using cut-off value of 0.50 m2 was 324 (20.1%) at aged 65 to 74 years, 202 (28.6%) at aged 75 to 84 years, 23 (29.1%) in more than 85 years. Among women older than 65 years prevalence of sarcopenia was 22.9% (Table 5).

Prevalence (%) of sarcopenia using cut-off of 0.49 m2 in geripausal women
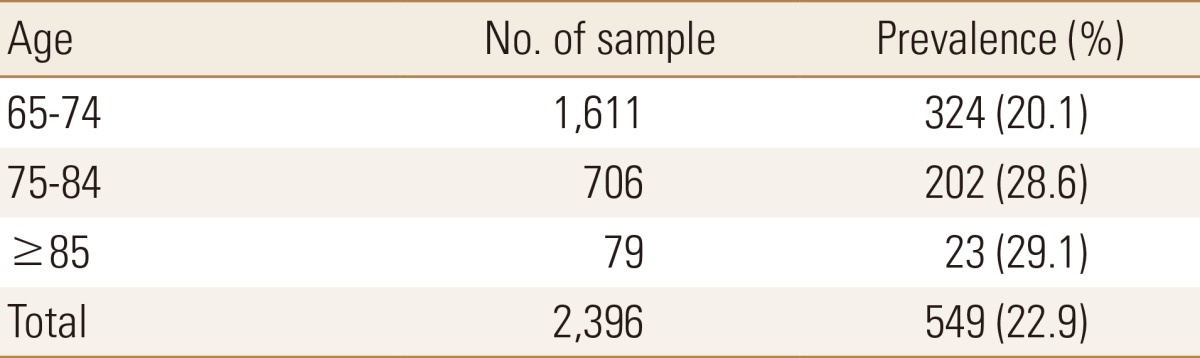
Prevalence (%) of sarcopenia using cut-off of 0.50 m2 in geripausal women
DISCUSSION
The present study evaluated the prevalence of sarcopenia in postmenopausal women using the cut-off point of ASM adjusted BMI (0.50 m2). This study showed that the overall prevalence was 15.6% in women 50 years and older and 22.9% in women 65 years and older.
Recently, the FNIH Sarcopenia Project proposed the most recent consensus on the definition and operational criteria for sarcopenia based on large and diverse population-based studies.[81213] They recommended ASM/BMI as a new operational method for calculating muscle mass.[13] They performed statistical classification and regression tree analysis to calculate the muscle mass index that is most strongly and directly correlated with weakness and slowness.[13] And they recommended 0.512 m2 as the cut-off value using ASM/BMI in women. However, we determined the cut-off point only by the distribution trend of ASM or ASM/BMI because that there are no evaluation on muscle function in KNHANES data. Nevertheless, the cut-off point that referenced the ASM/BMI was more corresponded with the cut-off point of FNIH than that of ASM.
A cross-sectional study in USA was performed 5,092 community-dwelling adults aged older than 60 years with grip strength (GS) data.[14] The objectives of this study were to determine the prevalence of muscle weakness using the FNIH sarcopenia project criteria and its relationship with physical limitations. Weakness prevalence using GS and GS with BMI definitions were 11.4% and 13.3% in women, respectively. And overall prevalence of physical limitations, basic ADL limitations and instrumental ADL limitations was 52.9, 28.1, and 35.9%, respectively. And other cross-sectional study was performed using International Mobility in Aging Study (IMIAS) involving 1935 community-dwelling older adults, between 65 and 74 years, who evaluated the hand GS (HGS) and gait speed assessment.[15] Weakness was defined according to sex-specific HGS cut points associated with slowness proposed by FNIH Sarcopenia Project. Weakness prevalence from Colombia and Brazil were 13.5 and 19.3% in women, respectively.
These findings correspond with our study. We found that the overall prevalence was 15.6% in women 50 years.
Our study has several limitations. First, we only considered low muscle mass when defining sarcopenia regardless of muscle function. Second, we did not exactly exclude women who have metabolic disease such as hyperthyroidism, diabetes mellitus, and other disease, which can influence the lean body mass.
Although the prevalence that was obtained by our study have little clinical evidence since the cut-off point that was used was not calculated by using our own cohort, the value we obtained is within the proper range of value to research about sarcopenia. Furthermore, using 0.50 m2 as the cut-off point can help compare various studies about sarcopenia in Korea.
Notes
This research was supported by a grant of the Korea Health Technology R&D Project through the Korea Health Industry Development Institute (KHIDI), funded by the Ministry of Health & Welfare, Republic of Korea (grant number, HC15C1189).
No potential conflict of interest relevant to this article was reported.