



INTRODUCTION
Muscle power and strength are the strongest predictors of the functional status of aged people. Muscular strength depends on muscle mass and neuromuscular function, which are deteriorated by aging-related muscle atrophy. Sarcopenia leads to aging-related reductions of muscle mass and strength, causing falls and fractures.[1-4] Sarcopenia reduces mechanical loading in the elderly and aggravates osteoporosis. Therefore, the bone and muscle interactions simultaneously deteriorate the muscles and bones, increasing the fragility fracture risk.[4-6] However, bone density and sarcopenia-induced decreased muscle strength is known to be improved by resistance exercise or concurrent aerobic and resistance training (RT)-induced muscular hypertrophy.[7,8]
The molecular basis of the hypertrophic response following the weight-bearing (resistance) exercise has been focused on the role of protein kinase B (PKB/Akt) and the mammalian target of rapamycin (mTOR) signaling-dependent protein synthesis.[9] Over-expression of PKB and/or the exercise-induced enhancement of mTOR have stimulated muscle hypertrophy and rescued muscular deterioration in animal denervation model.[10-12] Also, exercise training-induced muscular hypertrophy is accompanied by an increase of the myonuclei number in muscle fibers, which is responsible for the synthesis of the muscle protein.[13] During the resistance exercise, the satellite cells in the muscle fiber membranes are activated and fused to the existing muscle cells by adding extra nuclei,[14] and this mechanism facilitates mitochondrial biogenesis and dynamics.[15]
The main function of bones is to support skeletal muscles to maintain body posture and to allow physical activity. Thus, bone mass is a major determinant of muscle function.[16] Both weight-bearing resistance and running-based endurance exercise are dynamic and potentially osteogenic. However, while endurance exercise stimulates preferentially mitochondrial remodeling by enhancing mitochondrial biogenesis and dynamics, resistance exercise preferentially activates myofibrillar protein synthesis. Endurance exercise, such as jogging or walking, enhances moderately the loads on the skeleton above gravity, so it does not increase muscle cross-sectional area (CSA), which is directly related to muscle strength and power.[17,18] However, resistance exercise, such as weight training, is known to prevent the pathology of osteoporosis.[19,20] Therefore, a combination of walking and resistance exercise is expected to have a greater impact on muscle mass and bone structure or bone density than just walking.
The purpose of this study is to analyze the effects of walking and resistance exercises on the structure of bones, skeletal muscle mass, and bone mineral density (BMD) using national representative data.
METHODS
1. Ethics statement
Data from the 2008 Korean National Health and Nutrition Examination Survey (KNHANES), bearing the approval number 2008-04EXP-01-C, was reviewed and approved by the Institutional Review Board of the Korea Centers for Disease Control and Prevention (KCDC). Informed consent was obtained from all participants when the 2008 KNHANES was conducted.
2. Participants
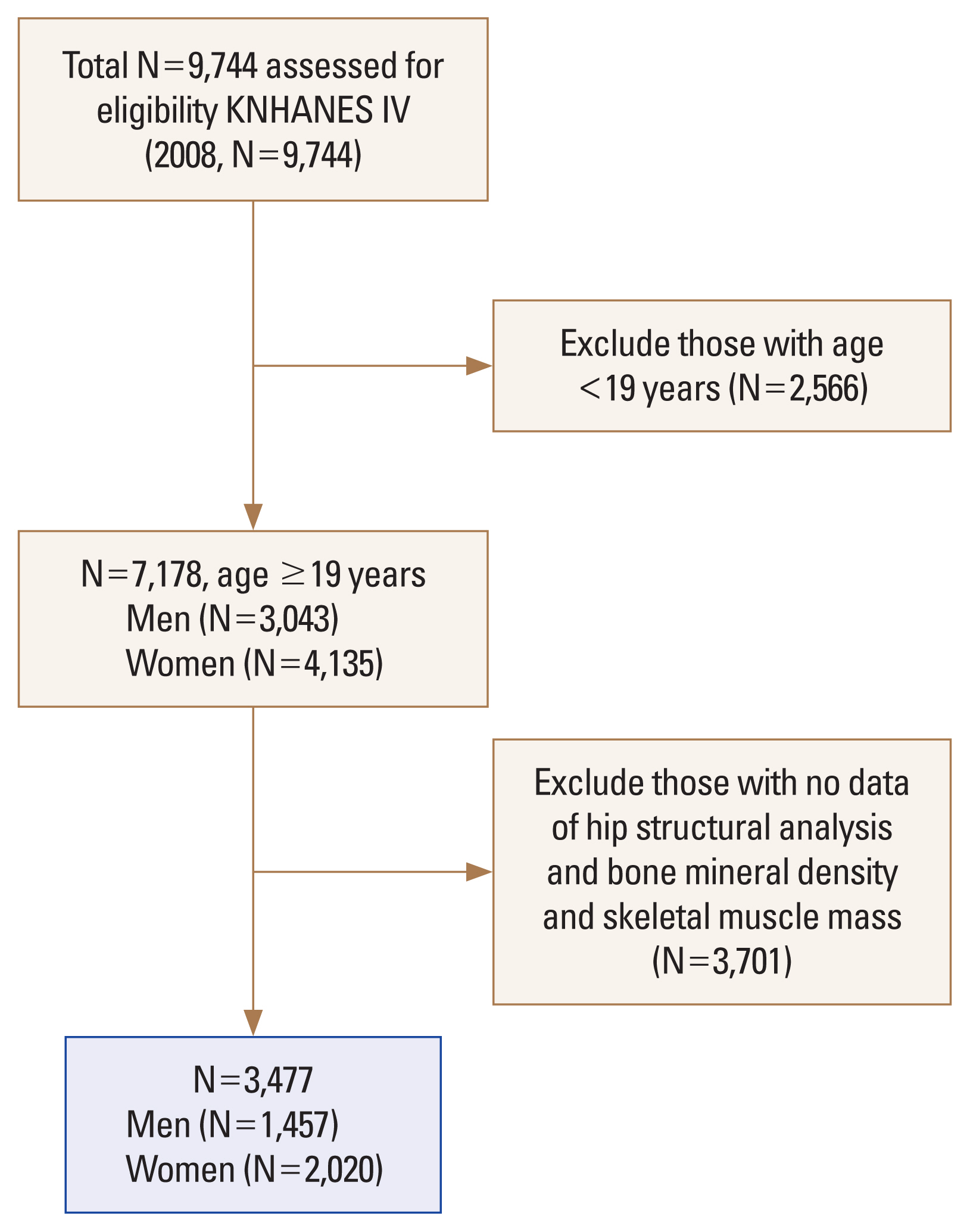
The KNHANES for the Korean population is a nationwide representative cross-sectional survey with a clustered, multistage, stratified, and rolling sampling design. The KNHANES consists of a health interview, health examination, and dietary survey. The survey data is collected from interviews and direct standardized physical examinations conducted in specially equipped mobile examination centers.[21] The data were collected in 2008 from 9,744 participants. Patients under 19 years of age (N=2,566) or patients without data on the skeletal-muscle-mass, BMD, and hip structural analysis (HSA) variables (N=3,701) were excluded. After these exclusions, 3,477 participants (1,457 men and 2,020 women) were finally analyzed (Fig. 1).
3. Materials
A health questionnaire was used to obtain information on the age, gender, socioeconomic status, and education status of each patient. Body weight and height were measured in light clothing with no shoes, and the body mass index (BMI) was calculated as the weight (kg) divided by the height squared (m2). Dietary intake was assessed by trained staff using a complete 24-hr recall method. The daily energy intake was calculated by referencing the nutrient concentrations of the foods according to the Korean Food Composition Table.[22]
4. Physical activity (Walking and muscle strengthening activity)
The KNHANES physical activity questionnaire was based on the Korean short version of the International Physical Activity Questionnaire (IPAQ).[23] Walking physical activity was defined as 5 or more days of walking per week for at least 30 min per day. The group that met the recommendation for walking activity engaged in such activity 5 days/week; those who did not meet the recommendation did so on ≤4 days/week. The muscle-strengthening activity was defined as 2 or more days of muscle-strengthening exercise per week for at least 30 min per day. Muscle-strengthening exercises include lifting weights, push-ups, sit-ups and squats. The group that met the recommendation for muscle-strengthening activity engaged in such activity more than 2 days/week; those who did not meet the recommendation did so on ≤1 day/week.
5. Measurements of the appendicular skeletal-muscle mass and BMD
Body composition was measured using whole-body dual energy X-ray absorptiometry (DXA), for which the QDR 4500A apparatus (Hologic Inc., Bedford, MA, USA) was employed. The bone mineral content, fat mass, and lean soft-tissue mass were measured separately for each part of the body, including the arms and legs; the lean soft-tissue masses of the arms and legs are nearly equal to the skeletal muscle mass. As absolute muscle mass is correlated with height, the skeletal muscle index (SMI) was calculated as follows: lean mass (kg)/height (m2). The arm SMI is defined as the arm lean mass (kg)/height (m2), while the leg SMI is defined as the leg lean mass (kg)/height (m2). The appendicular SMI is defined as the sum of the arm and leg SMIs.
BMD of femur intertrochanteric and at femoral neck (FN) and lumbar spine (L1-4) sites were measured by trained technicians using DXA.
6. HSA
To evaluate the hip-bone geometry, DXA scans were analyzed at the FN, and intertrochanteric region using the HSA program. The CSA, and cortical thickness (CT) were measured based on the bone-mass profiles, respectively.[24]
7. Statistical analyses
All subjects were analyzed based on age 65. To compare the means and proportions of each group, the Student’s t-test and the χ2 test were employed.
Hip structure, skeletal muscle mass, and BMD were compared between the exercise group. In addition, the sex, age, BMI, energy intake, and osteoporosis medication were adjusted when comparing the mean of the 2 groups. Then, non-activity group, only walking group, only muscle activity group, and walking and muscle activity group were divided into 4 groups. Likewise, hip structure, skeletal muscle mass, and BMD were compared between the 4 groups after adjusted covariates.
All statistical calculations were performed using SPSS Statistics version 22 (SPSS Inc., Chicago, IL, USA).
RESULTS
1. Demographic characteristics included present study
Of the 3,477 participants in this study, those age under 65 and those age 65 or more were 2,730 and 747, respectively. Height (P<0.0001), BMI (P<0.001), education (P< 0.001), and energy intake (P<0.001) were statistically significant differences between both age groups. Muscle-strengthening activity (P<0.001) and walking activity (P<0.001) were found to be statistically higher in those aged under 65 (Table 1). The incidence of osteoporosis was significantly higher in those aged over 65 (P<0.001). Physical activity was also significantly different in both age groups (P<0.001).
2. DXA findings by the walking activity
DXA finding demonstrated that BMD of femur neck (P= 0.003), intertrochanteric area (P<0.001) and lumbar spine (P=0.005) in a group of the age of 65 or older in which walking activity was performed with 5 days of walk or more per week for at least 30 min for each day were found to be significantly higher than that in the group in which walking activity was not performed with covariates concerned. DXA finding demonstrated that only SMI (P<0.001) in both age groups in which walking activity was performed with 2 days of muscle strengthening exercise or more per week for at least 30 min for each day were found to be significantly higher than that in the group in which muscle strengthening exercise was not performed following adjustment of covariates (Table 2).
3. DXA findings by the muscle resistance exercise
DXA finding demonstrated that BMD of intertrochanteric area (P=0.001) and SMI (P<0.001) in a group of the age of 65 or older in which muscle resistance exercise was performed with 2 or more days per week for at least 30 min for each day were found to be significantly higher than that in the group in which muscle resistance exercise was not performed following adjustment of covariates. In addition, DXA findings demonstrated that CSA of intertrochanteric area and CT of intertrochanteric area in a group of the aged under 65 in which muscle resistance exercise was performed 2 or more days per week for at least 30 min for each day were significantly higher than that in the group in which muscle resistance exercise was not performed following adjustment of covariates (Table 3).
4. DXA findings by presence of physical activity
DXA findings demonstrated that BMD of femur neck, intertrochanteric area and SMI in both age groups in which walking activity was performed with 2 days of muscle strengthening exercise or more per week for at least 30 min for each day were found to be significantly higher (P<0.001) than that in the group in which muscle strengthening exercise was not performed without covariates unconcerned. HSA findings demonstrated that SMI (P<0.001) in both age groups in which any level of activity was performed were found to be significantly higher than that in the group in which any level of activity was not performed while BMD of femur neck and intertrochanteric area were found to be significantly higher (P<0.001) in both age groups with any level of activity (Table 4).
DISCUSSION
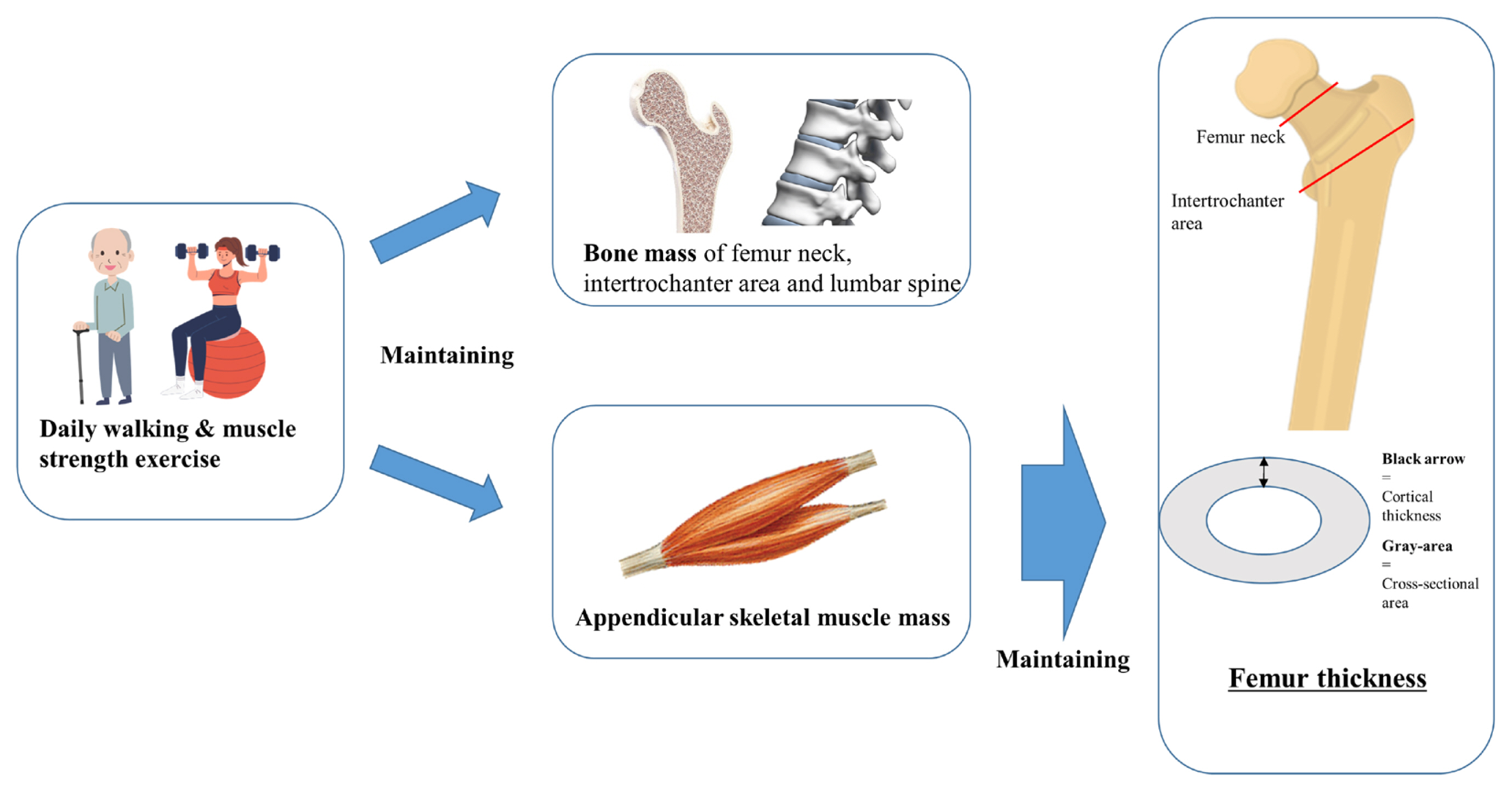
The principle findings of this study were that muscle mass and BMD are either increased or preserved in groups that have performed steady walking and muscle strength training. In addition, thickness and CSA of FN and intertrochanter were higher in elderly group compared to younger group in both long-term walking and muscle strength training (Fig. 2).
Yoshiko et al. [25] performed non-randomized controlled trial for quantifying the effects of walking and walking with home-based RT on the muscle quality of older individuals. They reported that the echo intensity of the quadriceps femoris was significantly decreased in both groups after training and improved muscle quality. Echo intensity of the quadriceps femoris was further decreased in the walking and home-based RT group compared with the walking training-only group. The sit-up test in both groups and the sit-to-stand and 5-m maximal walk tests in the walking group were significantly improved after training. Based on these results, they suggested that training-induced stimulation is associated with a decrease in echo intensity in some thigh regions. Furthermore, the addition of home-based RT to walking would be effective for a greater reduction of echo intensity.
In the present study, our results were corresponded that muscle mass was increased in group with steady walking and strength training. Beavers et al. [26] examined the effect of exercise modality during weight loss (WL) on hip and spine BMD in overweight and obese older adults. They performed analysis compared data from two 5-month, randomized controlled trials of caloric restriction (CR) with either RT or aerobic training (AT) in overweight and obese older adults. Participants in the RT + WL study underwent 3 days/week of 8 upper/lower body exercises (3 sets, 10 repetitions at 70% 1 RM) and participants in the AT+CR study underwent 4 days/week of treadmill walking (30 min at 65%-70% heart rate reserve). BMD at the total hip, FN, and lumbar spine was assessed via DXA at baseline and 5 months. They suggested that performing resistance, rather than aerobic, training during CR may attenuate loss of hip and FN BMD in overweight and obese older adults. In our study, the muscles showed an effective improvement in walking, but there was no difference in BMD according to the presence of walking activity. However, the difference in BMD was obvious in muscle strength exercise compared the walking exercise.
Beck et al. [27] performed the observational study using 6,032 women of mixed ethnicity aged 50 to 79 years who had DXA scans of the total body and hip. They reported that adjusted bone measurements showed similar activity effects with all 3 grouping variables, but these were greater and more significant when evaluated by lean body mass fraction (LMF) tertile. Women in the highest LMF tertile had the widest femurs. Differences in section modulus between the highest and lowest tertile of LMF were 50% to 80% greater than the association with bone mineral content and 2 to 3 times that on BMD. They suggested that more active women in the Women’s Health Initiative observational study had geometrically stronger femurs, although effects are underestimated, not apparent, or sometimes negative when using BMD as an outcome.[27]
A previous systematic review reported that performing resistance exercise 2 to 3 times a week for 1 year demonstrated the maintenance or increase of BMD at the lumbar spine and hip in postmenopausal women.[28] In a subgroup analysis of the Cochrane review and previous meta-analyses, resistance exercise has resulted in a significant improvement of BMD in the lumbar spine and femur neck in postmenopausal women.[29-31] A combination of resistance exercise and weight-bearing aerobic exercise (e.g., running, skipping, jumping, or high-impact aerobics) is recommended as resistance exercise training provides muscular loading while weight-bearing aerobic exercise provides additional mechanical loading to the bone above gravity. This combination has improved multiple musculoskeletal outcomes including BMD, muscle mass, and strength.[32-34]
Several studies have shown that resistance exercise and walking can affect osteoporosis and sarcopenia. There are also some reports that resistance exercise is related to bone strength. Nonetheless, we found that walking at least 30 min/day for more than 5 days a week and resistance exercise at least 30 min/day for more than 2 days a week can change bone structure important for fracture prevention. In particular, the strength of this study was to analyze the structure of bones, muscle mass, and BMD according to the intensity of exercise through the nationwide representative and analyzed the whole ages of 20s to 80s.
Several limitations need to be considered with respect to this study. First, its cross-sectional design does not allow for evaluation of the causality between the exercise and the bone and muscle; prospectively-designed studies are necessary to clarify this relationship. Second, the questionnaire was used to determine the degree of physical activity through exercise. Nevertheless, the validity and reliability of the Korean short version of the IPAQ used in this study have been verified through a number of studies. Future studies should demonstrate the relationship between objective indicators of exercise and musculoskeletal health. Third, because this study is a cross-sectional design, the patients’ past nutritional status and past exercise amount were not reflected in the study. In future studies, it is necessary to consider the past status of the participants.
CONCLUSIONS
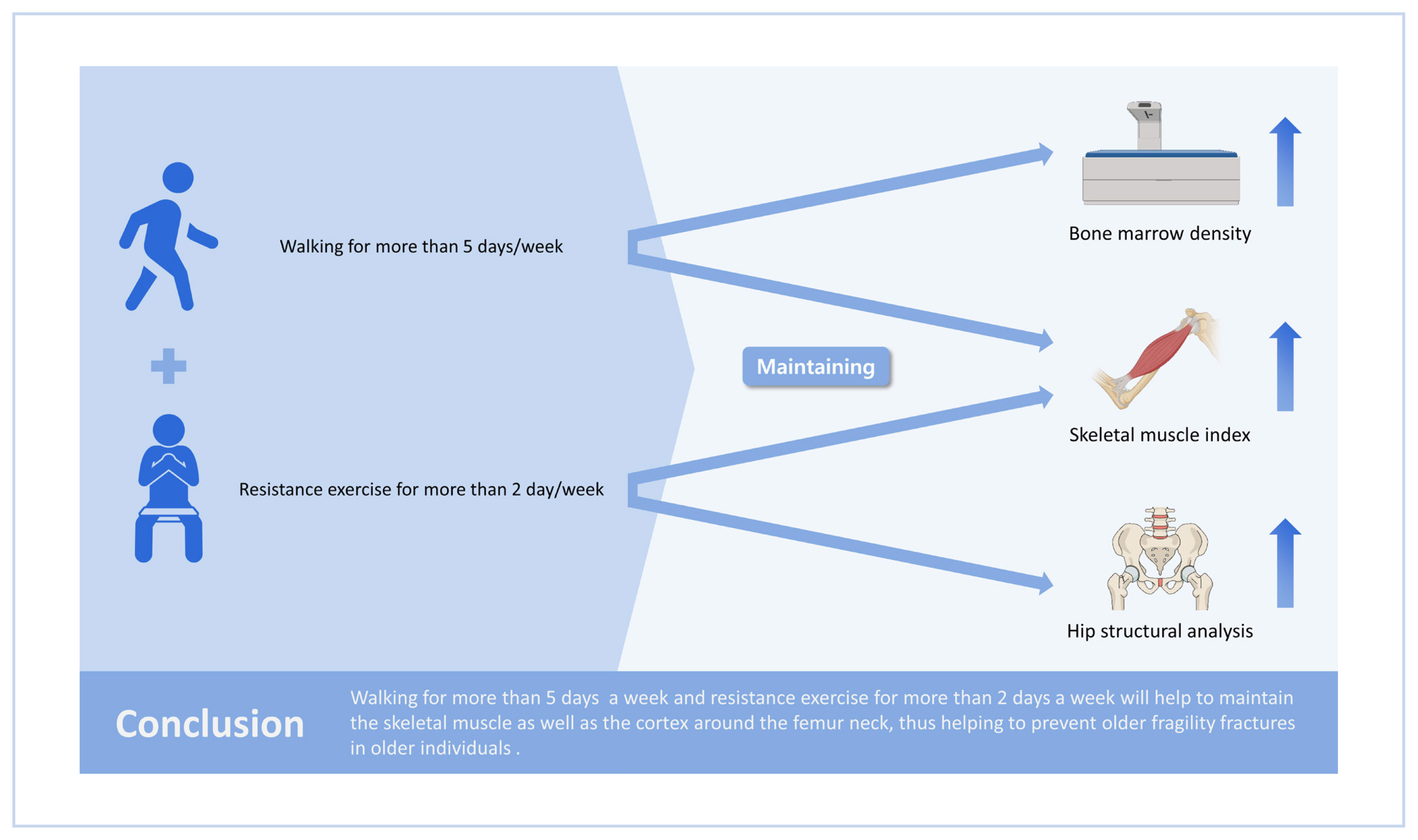
In conclusion, if accompanied by muscle strength exercise and walking, it will be possible to maintain bone and muscle loss and CT in the elderly. In particular, more than 5 days of walking per week and more than 2 days of muscle strengthening exercise will help to maintain the skeletal muscle as well as the cortex around the femur neck, thus helping to prevent older fragility fractures.
 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Print
Print






