The Role of Bisphosphonates Prior to Denosumab Treatment on Rebound Fractures: A Mini Review
Article information

Abstract
Denosumab is a potent anti-resorptive medication used to treat patients at high risk for osteoporosis; however, its beneficial effects on the skeletal system are quickly reversed after discontinuation. In contrast, bisphosphonates (BPs) are anti-resorptive agents with residual effects on the bone matrix; thus, these are capable of preserving bone mass for a long time. Therefore, subsequent anti-resorptive treatment with BPs is mandatory to prevent rebound fractures. Furthermore, BP administration before denosumab treatment appears to be a reasonable strategy for reducing hyperactivation of bone remodeling. In this review, we summarize the effects of BP administration before denosumab treatment in preventing rebound fractures after denosumab discontinuation.
INTRODUCTION
Anti-resorptive agents are still used as first-line treatment of osteoporosis.[1,2] Although denosumab (DMAB) can increase bone mineral density (BMD) and reduce fractures at all skeletal locations, its effects reverse quickly once treatment is discontinued.[3,4] Thus, strategies to prevent rebound fractures are urgently required. One of those strategies is the use of bisphosphonates (BPs).
In this review, we summarize the most recent evidence regarding the effects of BPs after, and especially before, DMAB treatment on several aspects of bone status to prevent rebound fractures after DMAB discontinuation.
METHODS
The study was conducted using relevant articles searched using Medical Subject Terms and Keywords (MeSH), such as DMAB discontinuation, rebound fractures, and prior BP use. These articles were included in PubMed and Cochrane library and were published in English up to September 2021. The term DMAB discontinuation was matched with the following terms: osteoporosis, BPs, rebound fractures, bone turnover markers (BTMs), and BMD.
We included cohort studies, case-control studies, cross-sectional studies, case reports, case series, and review articles that discussed prior BP use to rebound fractures after DMAB discontinuation. Non-English language publications, studies without primary outcomes relating to the main theme, or articles that cited DMAB as a treatment for other pathological conditions were excluded.
REBOUND FRACTURES AFTER DMAB DISCONTINUATION
BPs and DMAB are the most widely utilized treatments for postmenopausal osteoporosis. Both substances are anti-resorptive and function by slowing down the rate of remodeling and inhibiting osteoclastic activity, therefore preventing bone resorption.[1] BPs act by inhibiting farnesyl-pyrophosphate synthase, an important enzyme for osteoclast function and survival,[1] while DMAB is a monoclonal antibody with a high affinity for the activating receptor activator of nuclear factor-κB ligand (RANKL), preventing RANKL to bind to RANK.[5–7] Among the BPs, alendronate (ALE) and zoledronate (ZOL) can be absorbed into the bone matrix for a long time, thus having a residual and even permanent effect.[1,2]
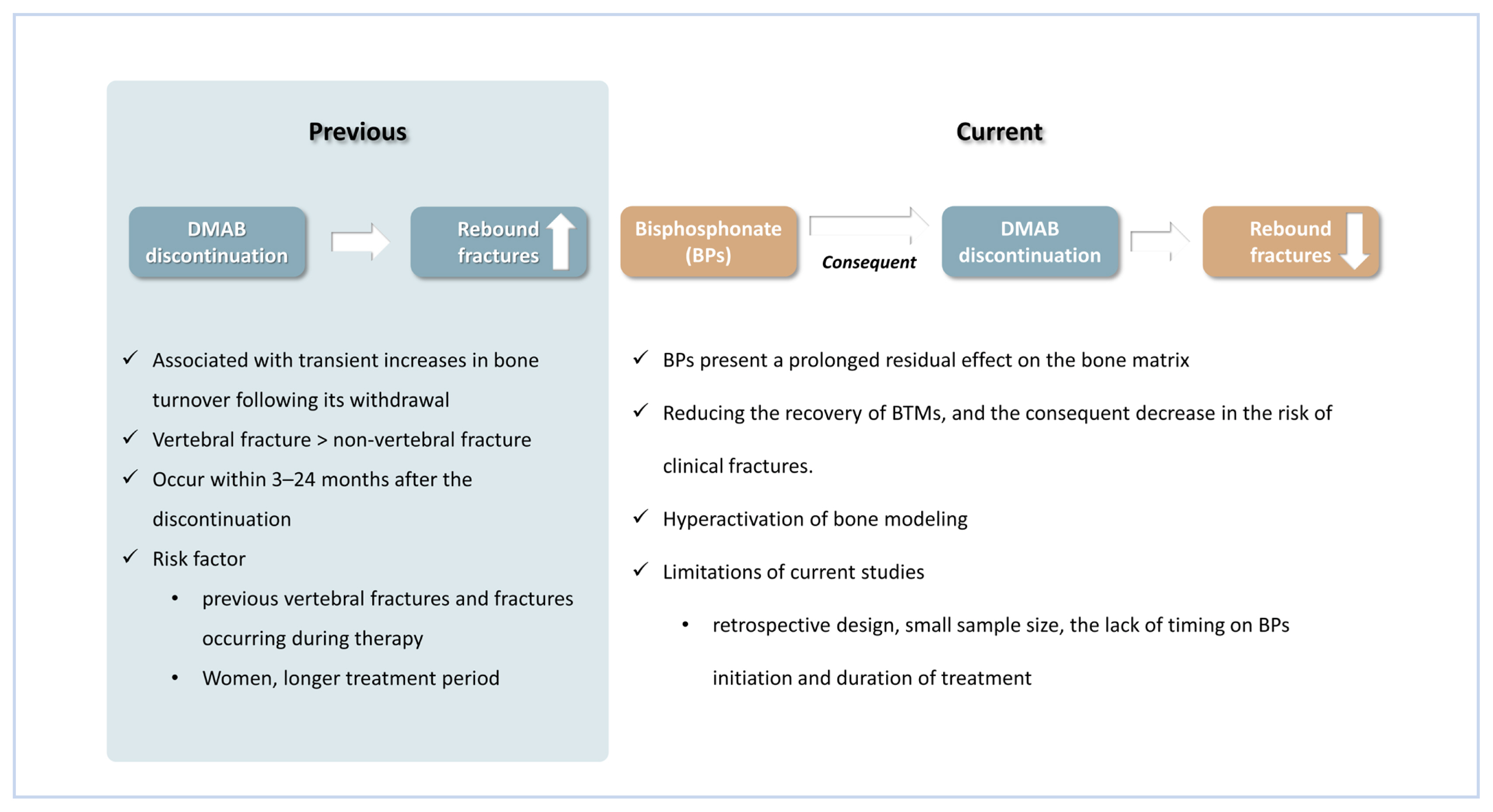
Although there have been reports of vertebral fractures linked with DMAB withdrawal in recent years,[8–18] the mechanism and risk factors for this phenomenon are still unclear. It is hypothesized that it may be associated with transient increases in bone turnover following its withdrawal,[5,8] resulting in a rebound effect on BTMs, with elevation above baseline and consequent decrease in BMD.[3,5,19]
Those rebound vertebral fractures after DMAB discontinuations are defined as new vertebral fractures associated with minimal trauma or even in the absence of trauma in the context of high bone turnover and rapid bone loss in the lumbar spine. They occur within 3 to 24 months after the discontinuation of a reversible anti-resorptive therapy in the absence of secondary causes of bone loss or fracture.[12]
The most critical period for fractures appears to be the first year of treatment discontinuation. The literature has documented rebound cases between 30 and 1,080 days after the last DMAB injection.[20,21]
Despite reports of multiple vertebral fractures, there is no apparent rise in non-vertebral fractures related to DMAB discontinuation. This could be explained by the fact that the trabecular bone has a faster rate of bone remodeling than the cortical bone, owing to it being more affected by excessive skeletal remodeling after DMAB discontinuation.[20,22] In patients with thin trabeculae, such as patients with osteopenia or osteoporosis, an increase in resorption depth relative to the thickness of the trabeculae may be the reason for the occurrence of a trabecular perforation.[22,23] As opposed to the trabecular bone, osteoclastic bone resorption occurs in tunnels in cortical bone and has shorter remodeling cycles.[24]
The most significant predictors of rebound vertebral fractures following DMAB discontinuation appear to be the occurrence of previous vertebral fractures and fractures occurring during osteoporosis therapy, both of which indicate an already compromised skeleton.[20] In the post hoc analysis reported in 2018, it was investigated if participants who discontinued DMAB during the FREEDOM study and FREEDOM Extensive Trial were at increased risk of developing new fractures or worsening current vertebral fractures.[4,25] Among the 1,471 participants (1,001 DMAB and 470 placeboes) who discontinued treatment (≥2 doses), the rate (95% confidence interval [CI]) of vertebral fractures increased to 7.1 (5.2–9.0) per 100 participants/year but was similar to the rate before and after discontinuation of placebo (7.0 [5.2–8.7] and 8.5 [5.5–11.5] per 100 participants/year, respectively).[4,25] However, the majority of fracture cases included high-risk participants who had previously experienced a vertebral fracture, and there was little information available on their previous treatments. The short follow-up period after treatment imposed restrictions on this analysis (median of 0.5 years).
Previously, it was believed that the risk of rebound increased with an increase in the number of DMAB doses applied. However, in a recent retrospective study of 797 patients, Burckhardt et al. [26] did not find the number of injections as a risk factor for a rebound. On the other hand, Lamy et al. [27] evaluated 5 case series and concluded that, after administering the second dose of DMAB, there was an increased risk of the rebound effect. Bone et al. [3] found that, in patients receiving DMAB for 2 years, the BMD values of the lumbar spine and total hip returned to baseline about one year after discontinuation of the medication. Women treated for a longer period (approximately 10 years) followed by discontinuation of DMAB experienced a reduction in total hip BMD that reached lower levels than the baseline.[28] There are also reports in the literature of patients who had vertebral fractures with discontinuation of DMAB after 2 injections, with no reports of fractures being identified after a single injection.[29]
THE ROLE OF BPs PRIOR TO DMAB TREATMENT
BPs may help maintain bone mass after DMAB discontinuation. The DATA follow-up study showed that patients receiving immediate anti-resorptive medication, either oral or intravenous BPs, retained the greatest gain in BMD after 4 years of DMAB therapy, which did not occur in a control group.[30] Kondo et al. [31] showed that ZOL had an advantage over BMD and BTM in patients who used DMAB for a maximum of 3 years. The preservation of bone mass gains with ZOL infusion after DMAB has also been reported in other studies [32] and there seems to be no difference between early or late administration of ZOL.[33] Thus, the benefit of an anti-resorptive therapy following DMAB in reducing the recovery of BTMs, and the consequent decrease in the risk of clinical fractures, appears to be well-established in the literature.[3,5,31–34]
However, only a few retrospective studies have evaluated the impact of BPs usage prior to DMAB on rebound fractures (Table 1). It has been suggested that the administration of BPs before treatment with DMAB also reduces BTMs, which consequently decreases the risk of rebound fractures.[3,35] Because some BPs present a prolonged residual effect on the bone matrix, they might contribute to the reduction of bone resorption that occurs after DMAB discontinuation, thereby reducing the risk of rebound fractures.[23]
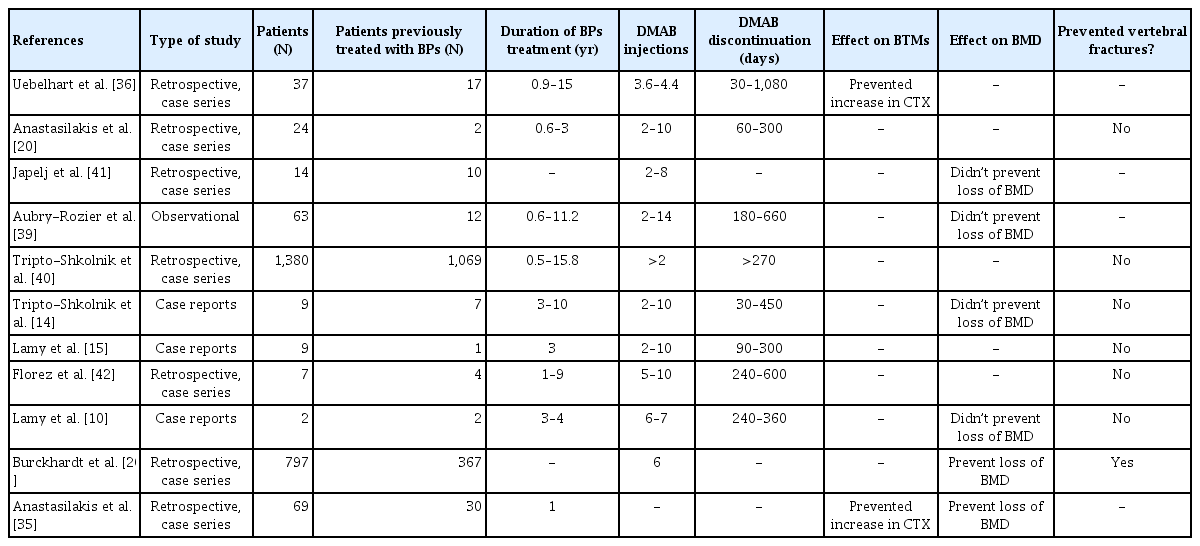
Studies that evaluated any effects of BPs treatment prior to DMAB on BTMs, BMD and vertebral fractures after DMAB discontinuation
In one study, 37 patients who had previously had BP treatment were retrospectively evaluated for BTMs. This was followed by sequential DMAB therapy.[36] The authors found lower serum C-terminal telopeptide (CTX) following DMAB discontinuation compared to patients who were not previously treated with BPs.[36] In another retrospective study, Anastasilakis et al. [35] found that the group who had taken ZOL for one year prior to DMAB had been able to suppress the increase of CTX up to one year. These findings reflect the rapid reversal of the biological effects of DMAB after its discontinuation and contrast with the residual skeletal effects of BPs.[24,37] Thus, monitoring BTMs following discontinuation of treatment would enable the identification of patients with a higher risk of vertebral fracture, thereby enabling the possibility of making better future therapeutic decisions.
However, regarding the prevention of bone loss after DMAB withdrawal, the benefits of prior BPs usage are still unclear. Six retrospective studies evaluated the effect of previous use of BPs on BMD in DMAB rebound [10,14,26, 38–40] but only one found an improvement in BMD with previous use of BPs.[26] The lack of details on BPs treatment duration and subsequent DMAB duration and number of injections given make these observations inconclusive (Table 1). For example, Aubry-Rozier et al. [39] conducted an observational study with 71 postmenopausal women to monitor the effects of BMD after DMAB discontinuation. However, 9% of patients had taken corticosteroids and about 23% had used aromatase inhibitors, which can be an important factor in increasing bone resorption.
Likewise, Tripto-Shkolnik et al. [14] reported a case series of high-risk patients with osteoporosis and multiple vertebral fractures after discontinuing DMAB despite prolonged prior exposure to BPs. Data were collected by phone from patients of different hospitals. They identified eight elderly women with multiple vertebral fractures, most spontaneous. The way the data were collected may well be subject to several information biases, including data on the time of BPs use, time since DMAB was stopped, and data on BTMs and BMD.[14]
In another retrospective study, Tripto-Shkolnik et al. [40] evaluated 1,380 postmenopausal women of whom 1,069 had used BPs for up to 15 years prior to the use of DMAB. The rate of osteoporotic fracture per 100 patients/year was higher in the group with previous use of BPs compared to the group without previous use, although the results were not statistically significant (relative risk, 1.67; 95% CI, 0.8–3.48).[40]
Burckhardt et al. [26] evaluated 797 patients who had discontinued the use of DMAB. The study aimed to assess risk factors for rebound and one of the conclusions was that prior treatment with BPs appeared to have only a small protective effect in preventing vertebral fractures compared to treatment after DMAB discontinuation. In this study, ibandronate was given in 27,3%, ALE in 25,7%, ZOL in 7,7%, and risedronate in 4,4%. However, there was no comparison between groups of patients with or without vertebral fractures, which limits the results of the study. In addition, only 47% of patients had previously used BPs and there were no details about treatment duration.
CONCLUSIONS
Rebound vertebral fractures after DMAB withdrawal is still a major concern. The studies on rebound fractures with DMAB according to previous BPs use have several limitations, including retrospective design, small sample size, the lack of timing on BPs initiation and duration of treatment. Considering these factors, it seems possible that BPs prior to DMAB could attenuate the hyperactivation of bone remodeling.
Acknowledgments
The authors would like to thank the entire UED-HAM (Unidade de Endocrinologia e Diabetes, Hospital Agamenom Magalhães), University of Pernambuco, Recife, Brazil, for providing us with the data and for allowing us to carry out the research.
Notes
Ethics approval and consent to participate
Not applicable.
Conflict of interest
No potential conflict of interest relevant to this article was reported.