


INTRODUCTION
Loss of muscle mass is a predominant change of body composition in elderly people. Rosenberg [1] defined age-related reduction of muscle mass as sarcopenia. Sarcopenia is characterized by decline in skeletal muscle mass and function that may result in reduced physical capability and poorer quality of life.[2,3] In recent years, the population of obesity is rapidly increasing. Aging and physical disability are also related to an increase in fat mass, particularly visceral fat,[4] an important factor in the development of metabolic syndrome and cardiovascular disease.
The concurrence of both obesity and sarcopenia, also known as sarcopenic obesity (SO), was first defined by Baumgartner [5]. It has been reported that SO can increase the risk of metabolic syndrome, physical disability, morbidity, and mortality compared to either sarcopenia or obesity alone.[6] The complex interplay of common pathophysiological mechanisms (such as increased proinflammatory cytokines, oxidative stress, insulin resistance, and hormonal changes) and decreased physical activity underlies the close relationship between sarcopenia and obesity.[7] Sarcopenia can reduce physical activity and total energy expenditure, thus increasing the risk of obesity.[8] In contrast, an increase in visceral fat induces inflammation which contributes to the development of sarcopenia.[9] The association between sarcopenia and obesity likely sets up a vicious cycle, resulting in further loss of muscle mass and mobility, insulin resistance, and risk of metabolic syndrome development.[10] For this reason, SO and its relation with other metabolic disease are important issues in elderly population. Furthermore, we hypothesized that there would be higher prevalence rate of sarcopenia within obesity due to that vicious cycle.
Korea is one of the most rapidly aging countries in the world.[11] Several studies have focused on the prevalence, etiology, and clinical issues of SO in Korea. However, the prevalence rates of SO were quiet different among studies. The objective of this study was to evaluate the prevalence of SO in large number of healthy Korean elderly women based on data of the Korea National Health and Nutrition Examination Survey (KNHANES) IV and V conducted in 2008 to 2011. We also compared prevalence rates of SO according to their obesity status.
METHODS
1. Study population
This study was based on data obtained from the KNHANES IV and V. The KNHANES is a nationally-representative survey conducted by the Korean Ministry of Health and Welfare. These surveys have been conducted periodically since 1998, using a rolling sampling design involving a complex, stratified, multistage, probability-cluster survey of a representative sample of the non-institutionalized civilian population in order to assess the health and nutritional status of the Korean population. Whole body dual energy X-ray absorptiometry (DXA) scan and body mass index (BMI) measurement were performed for individuals of ≥10 years old from July 2008 to May 2011(excluding pregnant women), individuals with a height of ≥196 cm or a weight of ≥136 kg were excluded in accord with the KNHANES survey protocol. In addition, test results were treated as missing value in participants with implanted radio-opaque material (e.g., a prosthetic device, implant or other radio-opaque object) that could affect DXA results. Postmenopausal women aged 65 years or more were included in this study. Written informed consent was obtained from all participants. Protocols for the KNHANES IV and V were approved by the Institutional Review Board of the Korean Center for Disease Control and Prevention.
2. Definition of sarcopenia and SO
Whole-body DXA examinations for the KNHANES study were conducted with a QDR4500A apparatus (Hologic Inc., Bedford, MA, USA). Data included values for bone mineral content (g), bone mineral density (g/cm2), fat mass (g), lean mass, bone mineral content (g), and fat percentage of the whole body and that of specific anatomical region. Appendicular skeletal muscle mass (ASM) was obtained by adding muscle masses of the four limbs by assuming that non-fat and non-bone masses were skeletal muscles. Skeleta mass index (SMI) was defined as ASM/height2. Asian Working Group for Sarcopenia (AWGS) suggested a classical approach to determine the cut-off value by using the value of two standard deviations below the mean for a young reference group which was 5.4 kg/m2 for women.[12] We used 5.4 kg/m2 as the cut-off value to determine the prevalence for sarcopenia among elderly Korean women.
BMI is commonly used to classify overweight and obesity in adults. According to the International Obesity Task Force recommendation, BMI categories were as follows: normal (between 18.5 and 23 kg/m2), underweight (<18.5 kg/m2), overweight (between 23 and 25 kg/m2), and obese (between 25 and 30 kg/m2).[13]
3. Statistical analysis
The χ2 test was used to compare categorical measures between groups defined by BMI. Odds ratios (ORs) and 95% confidence intervals (CIs) were estimated for the associations between obesity and sarcopenia using logistic regression analyses. All P-values of less than 0.05 were considered statistically significant. All analyses were conducted using SPSS software version 20.0 (SPSS Inc., Chicago, IL, USA).
RESULTS
In the elderly women, age was significantly higher in the sarcopenia group than the non-sarcopenia group (P<0.001). However, BMI (P<0.001), waist circumference (P<0.001), appendicular SMI (P<0.001), energy intake (P<0.001), and protein intake (P=0.001) were significantly lower in the sarcopenia group than the non-sarcopenia group (Table 1).
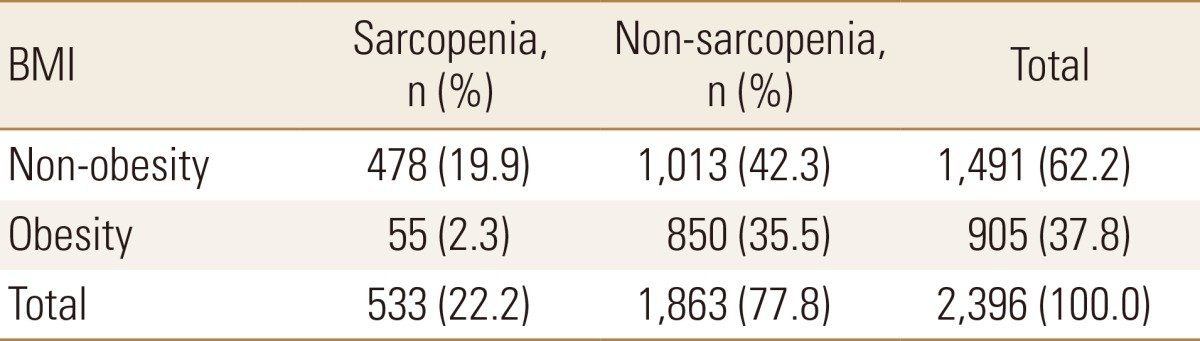
The 2008 to 2011 the KNHANES included 2,396 women ≥65 years (Fig. 1). Regarding age distribution, 1,611 were 65 to 74 years old, 706 were 75 to 84 years, and 79 were over 85 years. Among women over 65 years, 1,491 (62.2%) were underweight, normal weight, or overweight while 905 (37.8%) were obese (Table 2).
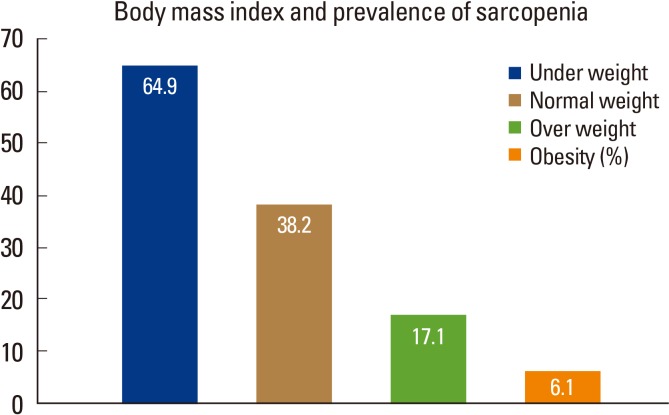
The prevalence of sarcopenia was 64.9% (63/97) in underweight women, 38.2% (320/838) in normal weight women, 17.1% (95/556) in overweight women, and 6.1% (55/905) in obese women (Fig. 2). The overall prevalence of sarcopenia among women ≥65 years was 22.2%. The prevalence of SO was 2.3% among elderly women ≥65 years (Table 2). Participants with BMI of 25 or above had lower odds of having sarcopenia (OR, 0.14; 95% CI, 0.10-0.18; P<0.01) than those with BMI <25.
DISCUSSION
This study evaluated the prevalence of SO in healthy elderly women in Korea. The results showed that the overall prevalence of SO was 2.3% in women of 65 years or older. The prevalence of sarcopenia was different among groups according to BMI. The prevalence rate of sarcopenia in obese women was lower than that in non-obese women.
To clarify the definition of sarcopenia, various working groups have published consensus papers. We addressed the prevalence of sarcopenia using 5.4 kg/m2 as recommended value by the AWGS. We also defined obesity as BMI ≥25 according to the International Obesity Task Force recommendation.
The prevalence of SO significantly differed from those of previous studies,[6,14,15,16,17,18,19,20,21,22,23,24] ranging from 0% to 48% depending on the background of the studied population, parameters, and cut-off values used for muscle volume quantification. Furthermore, methods and cut-off values used to define obesity were different among these studies. In this study, the prevalence rate of SO was lower than other previous studies. In general, SO prevalence is lower using height adjusted SMI compared to weight or BMI adjusted SMI. This phenomenon is prominent in Korea because differences in height between age groups are greater among Koreans compared to those in other countries.[25] Moreover, SO prevalence is higher using % body fat compared to that using BMI as a parameter of obesity.[26] In this study, we used height adjusted SMI and BMI as a parameter of SO. This might have resulted in lower prevalence of SO compared to that in other previous studies.
Patients with obesity were at decreased risk of prevalent sarcopenia in this study. This finding is consistent with findings of others. In a previous cohort study, low BMI was a risk factor for both current and future sarcopenia in very old age. The prevalence and incidence of sarcopenia were high in the underweight group in the present study. Low BMI might be a reasonable proxy for low lean mass.[27] Previously, BMI has been found to be the only predictor of skeletal muscle mass for women.[27] It is strongly and negatively correlated with the prevalence of sarcopenia.[28]
Although BMI is commonly used as a surrogate parameter for obesity, it indicates weight-for-height without considering differences in body composition or contribution of body fat to overall body weight. The mass of muscle is reduced while that of fat tissues is increased in the elderly. Thus, BMI might be a poor marker of body fat because it does not distinguish between fat and lean body mass, especially in old ages. This is a kind of “Obesity Paradox” commonly mentioned in heart failure, cardiovascular disease, and other chronic diseases.[29]
SO is a novel concept that has become more important in the elderly population. However, different definitions of sarcopenia and SO limit the discovery of clinical application of this disease with regard to other metabolic diseases and cardiovascular diseases. Therefore, consensus definition needs to be established for SO to promote standardized diagnosis and management for this disease in future study.
This study has several limitations. First, we only considered low muscle mass when defining sarcopenia regardless of muscle function. Second, we did not specifically exclude women with metabolic diseases such as hyperthyroidism or diabetes mellitus that might influence lean body mass.
This study has several powerful strengths. A large number of participants were included and analyzed by using data obtained from the KNHANES. Furthermore, the data of the KNHANES are representative of the entire Korean population. To the best of our knowledge, this is the first study addressing the prevalence of sarcopenia using 5.4 kg/m2 as recommended value by the AWGS in Korea.
In conclusion, the prevalence rate of sarcopenia in obese women was lower than that in non-obese women. We examined the prevalence of SO in Korean elderly women by using AWGS recommendation. The prevalence of SO was lower compared to other previous studies because of different method to define it. A consensus definition of SO needs to be established.


 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Full text via PMC
Full text via PMC Download Citation
Download Citation Print
Print






