Proton-pump Inhibitor Use and Fracture Risk: An Updated Systematic Review and Meta-analysis
Article information
Abstract
Background
This study's objective was to evaluate the association between proton-pump inhibitor (PPI) use and bone fracture incidence and bone mineral density (BMD) by meta-analyzing the estimates reported by epidemiological and cohort studies.
Methods
Data were acquired from studies identified after a literature search in electronic databases. Odds ratios (ORs), hazard ratios (HRs), and risk ratios (RRs) between PPI use and bone fracture incidence were pooled under the random effects model, and meta-analysis of standardized mean differences between PPI users and controls in cross-sectional values and BMD changes was conducted.
Results
Thirty-three studies fulfilled the eligibility criteria. These studies provided data from 2,714,502 individuals with a mean age of 66.91 years (95% confidence interval [CI], 63.37–70.46); 33.21% (95% CI, 30.44–35.99) were males and 64.61% (95% CI, 60.73–68.49) were females. Overall, fracture incidence was 22.04% (95% CI, 16.10–27.97) in PPI users and 15.57% (95% CI, 12.28–18.86) in controls. The overall effect size of the point estimate was 1.28 (95% CI, 1.22–1.35) between PPI use and bone fracture incidence. There was a trend towards increased fracture incidence from short duration use: OR 1.29 (95% CI, 1.19–1.40), medium duration use: OR 1.33 (95% CI, 1.12–1.55) and long duration use: OR 1.62 (95% CI, 1.33–1.90). There was no significant difference in the standardized mean differences between PPI users and controls, either in cross-sectional BMD values or in the BMD change observed in longitudinal studies.
Conclusions
Pooling of ORs, HRs, and RRs suggested that PPI use might increase fracture risk. However, there was no effect of PPI use on BMD.
INTRODUCTION
Proton-pump inhibitors (PPIs) are widely prescribed medications used to treat acid-related gastrointestinal diseases and are considered the superior option for anti-secretory therapy against several conditions including: non-erosive gastrointestinal reflux disease, erosive esophagitis, dyspepsia and peptic ulcer in terms of improved symptomatic outcomes [1] and as co-therapy with non-steroidal anti-inflammatory drugs for the prevention of peptic ulcers.[2] PPIs irreversibly block the proton pump (H+-K+-ATPase ion exchanger) in the stomach's acid-secreting parietal cells, leading to a profound inhibition of gastric acid secretion.[3]
In general, PPIs are well tolerated with minimal short-term side effects; therefore, these drugs are considered safe therapeutic regimens.[4] However, many epidemiological and cohort studies have observed an association between PPI use and an increased fracture risk among long-term PPI users,[5] which has raised concerns about their long-term use, especially in individuals with fracture risk. This risk is concerning for patients who prescribe PPIs and wish to balance their efficacy and the possibilities of future metabolic bone disease and fracture.[6]
Whereas many studies have found significant associations between PPI use and fracture risk, others could not endorse these findings. This discrepancy has necessitated a comprehensive review of the literature to synthesize the evidence. Recently, a meta-analysis of relative risk obtained from 18 studies found a modest risk of bone fractures with PPI use.[7] We conducted a systematic review and performed a meta-analysis by including all possible sources of prospective and retrospective data to evaluate the relationship between PPI use and fracture incidence.
METHODS
The present study was performed following the Cochrane Collaboration guidelines for conducting systematic reviews and meta-analysis, and the Preferred Reporting Items for Systematic Reviews and Meta-analysis (PRISMA) statement was used as guideline for preparing the present report.
1. Eligibility criteria
Inclusion criteria: (1) the study was general/patient population-based prospective or retrospective examining the association between PPI use and fracture incidence; (2) the study reported fracture incidence (hip, femur, forearm, hindarm, humerus, spine, etc.) in PPI users vs PPI non-users or the odds or hazards of using PPI for fracture incidence; (3) the study reported PPI use in individual with and without fracture incidence; or (4) the study reported either the epidemiological value of bone mineral density (BMD) or the BMD change in PPI users and their non-user controls. Exclusion criteria: (1) the study examined the association between fracture incidence and PPI use in combination with other drugs such as histamine2-receptor antagonists; or (2) the study involved other related measures such as falls or fracture-related mortality but not fractures per se.
2. Literature search
The literature search was conducted in electronic databases including: PubMed, Embase, and Google Scholar using the following relevant keywords and subject headings: PPIs, lansoprazole, dexlansoprazole, rabeprazole, pantoprazole, omeprazole, bone density, fractures, incidence, humans, medical records, BMD, incidence, hazard, odds, cohort, case-control, prospective, retrospective, database, general population, patient population, registry, medical records, trial, and registries. The search encompassed articles published in peer-reviewed journals in the English language before February 2018. Each database was searched for the aforementioned search terms. The search encompassed articles published in peer-reviewed journals in the English language before February 2018. Additional searches included the considerations of software-suggested corroborations and cross references of important research papers and review articles relevant to the present study.
3. Meta-analysis endpoints
For the present study, the meta-analysis endpoint was the attainment of a point estimate by pooling the odds ratio (OR), hazard ratio (HR), and risk ratio (RR) between PPI use and fracture incidence reported in individual studies. Subgroup meta-analysis were performed regarding low/medium/high PPI use, short/medium/long duration PPI use, outcomes of prospective vs. retrospective studies, and the fracture site. An additional endpoint was differences in cross-sectional values of BMD and BMD changes between PPI users and non-users observed in longitudinal studies.
4. Data and analyses
Demographic and clinical characteristics of subjects, study characteristics, and outcomes were extracted from respective research articles using a standardized procedure and were organized in specialized datasheets. Meta-analysis were performed using a random-effects model with STATA software (version 12; Stata Corp., College Station, TX, USA) by pooling the OR, HR, and RR reported by individual studies to achieve the overall effect size (OR approximated RR). The classifications used either for low, medium, and high intensity or for short, medium, and long duration were those of individual studies' authors which are reported in Table 1.
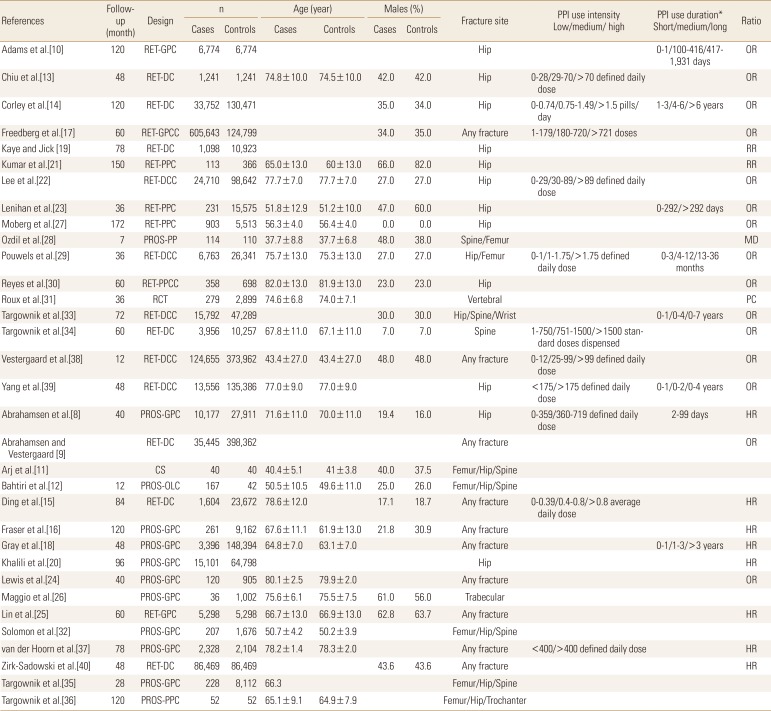
Characteristics of the included studies which recruited cases with fractures and non-fracture controls
For the assessment of the relationship between PPI use and BMD, meta-analyses of standardized mean differences (SMD) were performed by using RevMan software (version 5.3.1; The Cochrane Collaboration, Oxford, UK) to evaluate the significance of differences in BMD between PPI users and non-users or change in BMD after PPI use reported by longitudinal studies.
The overall effect size/s in the meta-analysis were a weighted average of the inverse variance adjusted individual effect sizes. Between-study inconsistency was tested using the I2 index. For the assessment of publication bias, Begg's funnel plot asymmetry tests was performed, and trim-and-fill method was used to estimate the number of missing studies. All data are presented as weighted effect sizes with 95% confidence interval (CI) and P<0.05 were considered statistically significant.
RESULTS
Thirty-three studies [8-40] fulfilled the eligibility criteria (Fig. 1). No significant publication bias was detected with the Begg's test of funnel plot asymmetry (adjusted Kendall's score=58±40.32; P=0.15), but the trim-and-fill method indicated the possibility of up to 4 missing studies (Supplementary Fig. 1). Important characteristics of these studies are presented in Table 1. Study subjects had a mean age of 66.91 years (95% CI, 63.37–70.46). Thirty-three point twenty one percent (95% CI, 30.44–35.99) were males while 64.61% (95% CI, 60.73–68.49) were females. Overall, fracture incidence was 22.04% (95% CI, 16.10–27.97) in 302,522 PPI users and 15.57% (95% CI, 12.28–18.86) in 833,254 controls (data from 14 studies).

A flowchart of study screening and selection process after the literature search.
1. Relationship between PPI use and fractures
For the point estimation of the relationship between PPI use and fracture risk, pooling of the OR, HR, and RR revealed an effect size of 1.28 (95% CI, 1.22–1.35) (85 ratios from 2,714,502 individuals; I2=89.7%; P<0.00001; Supplementary Fig. 2). The follow-up duration was 73.12 (95% CI, 60.70–85.54) months (range, 12–150 months; data from 23 studies). There was a trend toward increased fracture incidence from short duration use, pooled OR 1.29 (95% CI, 1.19–1.40); I2=69.1%; P=0.001) to medium OR 1.33 (95% CI, 1.12–1.55); I2=86.6%; P<0.00001) and long duration use OR 1.62 (95% CI, 1.33–1.90); I2=71.7% ; P<0.00001) (Fig. 2). There was no difference in fracture incidence with low OR 1.22 (95% CI, 1.078–1.36); I2=91.9%; P<0.00001), medium OR 1.32 (95% CI, 1.08–1.56); I2=91.3%; P<0.00001) and high PPI use OR 1.26 (95% CI, 1.045–1.47); I2=91.1%; P<0.00001; Fig. 3).
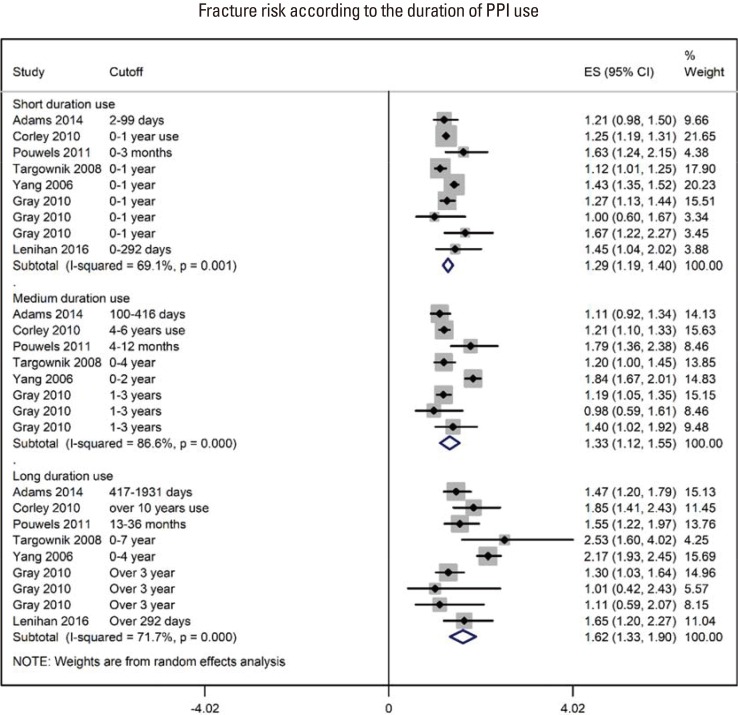
A forest graph showing the outcomes of a subgroup meta-analysis conducted to evaluate the effect of proton-pump inhibitor (PPI) use on fracture incidence with respect to the duration of PPI use. ES, effect sizes; CI, confidence interval.

A forest graph showing the outcomes of a subgroup meta-analysis conducted to evaluate the effect of proton-pump inhibitor (PPI) use on fracture incidence with respect to the intensity of PPI use. ADD, average daily dose; DDD, defined daily dose; SDD, standard daily dose; PDC, proportion of days covered; ES, effect sizes; CI, confidence interval.
In other subgroup analyses, the effect sizes of the OR, HR and RR between PPI use and fracture incidence were OR 1.33 (95% CI, 1.25–1.41); (I2=92.4%; P<0.00001; 57 OR from 14 studies), HR 1.26 (95% CI, 1.19–1.33); (I2=49%; P=0.005; 23 HR from 8 studies), and RR 0.74 (95% CI, 0.48–0.99); (I2=43.1%; P=0.134; 5 RR from 2 studies), respectively (Supplementary Fig. 2). Outcomes regarding the study design were similar for retrospective studies OR 1.29 (95% CI, 1.21–1.36); (I2=91.5%; P<0.00001; 18 studies) and for prospective studies OR 1.27 (95% CI, 1.16–1.38); (I2=49.7%; P=0.009; 7 studies). Effect sizes regarding the fracture site were hip with OR 1.34 (95% CI, 1.24–1.46); (I2=89.6%; P<0.00001; 15 studies), spine OR 1.18 (95% CI, 0.93–1.42); (I2=91.5%; P<0.00001; 10 studies), and any fracture OR 1.24 (95% CI, 1.18–1.31); (I2=78.6%; P<0.00001; 22 studies).
2. Relationship between PPI use and BMD
In the literature search, 11 studies were identified that reported the association between PPI use and either the cross-sectional BMD values or the BMD changes evaluated in longitudinal designs. Overall, data for 1,863 PPI users and 34,392 controls were used in this meta-analysis.
With respect to the cross-sectional BMD values, there was no significant difference between the PPI users and their non-user counterparts (SMD, 0.00; 95% CI, −0.18 to 0.19; P=0.96; I2=72%; P=0.0002; Fig. 4A). Also, there was no significant difference between PPI users and PPI non users in the BMD changes observed in the longitudinal studies (SMD, 0.07; 95% CI, −0.06 to 0.20; P=0.32; I2=80%; P<0.00001; Fig. 4B). In these studies, treatment durations were between 1 and 8 years.
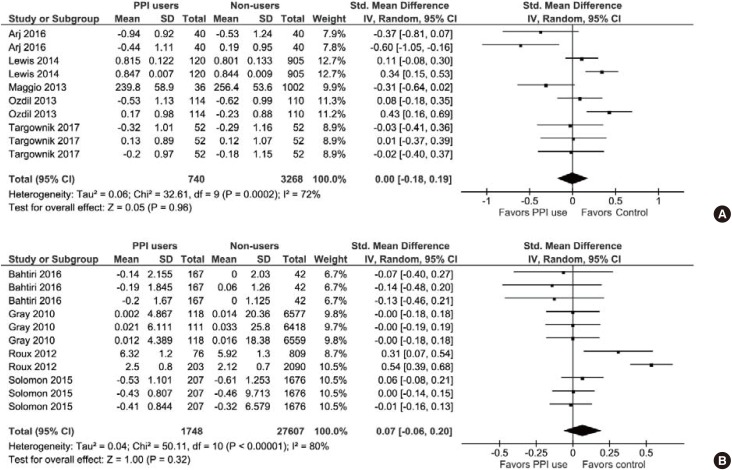
(A) A forest graph showing the meta-analysis of standardized mean differences between proton-pump inhibitor (PPI) users and non-users in cross-sectional bone mineral density (BMD) values observed in individual studies. (B) A forest graph showing the meta-analysis of standardized mean differences between PPI users and non-users in the BMD changes observed in longitudinal studies. SD, standard deviation; CI, confidence interval; df, degrees of freedom.
DISCUSSION
In this meta-analysis, we found that PPI use might increase fracture risk. A subgroup analysis also showed that the risk of fracture incidence with PPI use increased from short duration use to medium through high duration use. However, there was no significant difference between the PPI users and their non-user counterparts, either in cross-sectional values of BMD or in the change in BMD observed in longitudinal studies. At least 12 of the included studies failed to observe a significant association between PPI use and fracture incidence or BMD.
So far, a mechanistic relationship between PPI use and fracture incidence is lacking. However, many factors are identified that can affect this relationship. PPI therapy may be associated with side effects such as vitamin B12 deficiency, hypomagnesaemia, Clostridium difficile infection, pneumonia, gastrointestinal and cardiovascular risks [4142] and may also interfere with bioavailability and/or metabolism of minerals such as calcium, iron and magnesium.[43] A review has also found that PPI use is associated with increased risk of chronic kidney disease.[44] Whereas in vitro studies have shown deleterious effects of PPIs on bone cells possibly by affecting bone turnover,[45] in vivo studies have shown that PPIs inhibit osteoclast mediated resorption when delivered to a bony defect in self setting calcium phosphate cements.[46] Bone fragility depends not only on areal BMD but also on other factors including bone quality, which may be affected by other factors such as vitamin B12 levels and modulated skeletal fragility due to collagen cross-linking independent of areal BMD.[47]
Although these results suggest that PPI therapy increases fracture risk, confounding factors may play a role in the overall outcomes. Participant age in individual studies ranged from 38±9 to 82±13 years, for example. Effects of aging, general health conditions and comorbid conditions may affect the actual prevalence of fractures. This presumption is further supported by the fact that PPI use had no effect on BMD. Many drugs, such as antipsychotics, anti-Parkinson's and anti-seizure medications can affect bone strength and are associated with increased fracture risk.[39] Thyroxine replacement therapy and warfarin may also affect the incidence rate of fractures.[4849] Thus, possible spurious effects of confounders can't be ruled out when interpreting the results of this meta-analysis. Delineation of such effectors may be possible in the future as confounder variable-specific analyzable data from future trials become available or further retrospective analyses are performed.
In the present meta-analysis, the majority of fracture cases were related to the hip. Hip fractures can have several determinants. Falls, muscle weakness, low physical activity levels, suboptimal nutrition, drugs increasing fall risk and comorbid conditions of the neuromuscular system may contribute to hip fracture disability.[50] Neurological and neurodegenerative diseases such as Alzheimer's disease also pose significant fracture risk.[51] These factors may contribute to the presence of high statistical heterogeneity in the meta-analysis.
A significant increase in cardiovascular disease (CVD) incidence has been found with PPI use.[52] Some studies have also reported an increased incidence of major adverse cardiac events in patients who received PPIs along with an antiplatelet drug, clopidogrel.[5354] A recent meta-analysis has also found that co-prescription of PPI and thienopyridines increases the risk of ischemic and composite stroke.[55] In the present study, four of the included studies reported incidence of CVD events, which was almost double OR 1.90 (1.52–2.37); P<0.00001) in PPI users (n=20,268) compared with non-users (n=21,298). However, the possible influence of confounding factors in the association between PPI use and increased cardiovascular risk cannot be ruled out [56] because fracture incidence has been found to be usually higher in patients with comorbidities,[575859] which could be partially related to physical inactivity following fracture.[60]
There were several limitations to this study. There were a large number of studies included in this meta-analysis and were primarily observational rather than randomized controlled trials. This is the evidence currently available on this topic. Also, in subgroup analysis of the present study, outcomes were mostly associated with moderate to high I2. Sources of statistical heterogeneity could be several but usually originate from clinical and methodological heterogeneity. Clinical heterogeneity may arise from patients' differences, interventions or co-interventions and outcome measures, whereas the methodological heterogeneity may arise from the use of different study designs, cut-offs, and control over bias.
Regardless of the possible impacts of unidentified factors, the outcomes of the present meta-analysis demand a judicious and cautious use of PPIs. Studies have found that inappropriate use of PPIs in the inpatient setting is prevalent and should be discouraged.[61] With some caveats, authors of previous meta-analysis have also suggested that there could be a potential association between PPI use and fracture incidence especially hip and vertebral fractures.[762] Moreover, a strong association has been reported between PPI use and the subsequent prescribing of anti-osteoporotic drugs. Such an association has been also found to increase in a dose and time dependent manner.[63] Patients requiring continuous PPI therapy should ensure the recommended daily intake of calcium and vitamin D. However, the pharmacologic osteoprotection or BMD monitoring may not be advisable for chronic PPI users unless other indications necessitate it.[64]
CONCLUSIONS
Data generated from prospective and retrospective studies may be used for better statistical modeling to study potential confounding factors [5] and by arranging more homogeneous sub-datasets. Risk stratification of elderly, frail, malnourished, dialyzed and chronically hospitalized patients will also help in narrowing the conclusive evidence.[43] Prospective studies should establish cohorts of long-term PPI users and their non-user controls to follow BMD changes.[64] Even more useful, although potentially more demanding, would be to conduct randomized controlled trials.[5]
Notes
No potential conflict of interest relevant to this article was reported.
References
SUPPLEMENTARY MATERIALS
Supplementary Fig. 1
Forest graph showing the outcomes of an overall pooling of all odds ratios, hazard ratios, and relative risks for point estimation depicting relationship between the proton-pump inhibitor (PPI) use and the incidence of fracture. DDD, defined daily dose; SDD, standard daily dose; PDC, proportion of days covered; ES, effect sizes; CI, confidence interval.
Supplementary Fig. 2
A funnel plot showing the outcomes of trim and fill method of publication bias assessment. Theta represents the effect sizes of point estimate ratios.