


INTRODUCTION
Osteoporosis has become a major public health issue. It is rapidly increasing globally, especially in elderly Asians.[1,2,3] The projected incidence of hip fracture in Asia will account for 37% of all hip fractures worldwide by 2025.[4] The prevalence of osteoporosis in Korean women older than 50 years has been reported 35.5% from the Korean National Health and Nutrition Examination Survey (KNHANES) [5] and 24.3% from a recent regional cohort study (Ansung cohort).[6]
Calcium and vitamin D are an essential nutrient in maintaining optimal bone health. Appropriate doses of calcium and vitamin D intake were shown to be pharmacologically active, safe, and effective for the prevention and treatment of osteoporotic fractures.[7,8] Therefore, several guidelines for osteoporosis have recommended increased daily calcium and vitamin D intake to prevent and treat osteoporosis.[9,10,11,12,13] The recommended calcium and vitamin D intake varies according to age. In Korea, the daily calcium and vitamin D intake is recommended as approximately 700 mg and 10 µg, respectively, for women over 50 years of age.[14] However, the calcium intake of Korean women is reportedly only 55.2% of the dietary reference intakes for Koreans (KDRIs).[14] Vitamin D insufficiency is also very common in the general population,[15] but no data on vitamin D intake are available. Moreover, studies on the dietary intake of calcium and vitamin D among osteoporotic fracture patients are limited.
In this cross-sectional study, we evaluated the prevalence of low calcium and vitamin D intake using a self-reporting questionnaire, evaluated the associated factors of low intake, and determined the effect of calcium and vitamin D intake on bone mineral density (BMD) in patients with osteoporotic fracture.
METHODS
1. Study participants
From January to July 2015, 277 women were enrolled in this multicenter, hospital-based cross-sectional study on osteoporotic fracture. Fourteen hospitals participated. Inclusion criteria were female sex, fall-related osteoporotic vertebral, hip, and wrist fractures, age 50 years or older, and voluntary willingness to answer the questionnaire. Exclusion criteria were pregnancy, high-energy trauma, pathologic fracture secondary to metastasis, dementia and inability to be interviewed. The study was approved by the ethics committee in each hospital. Participants signed informed consent to participate in the study.
2. Assessment of dietary calcium and vitamin D intake
To evaluate dietary calcium and vitamin D intake, the Korean Calcium Assessment Tool (KCAT) self-reported questionnaire was used. KCAT is a simple and convenient questionnaire developed based on the Calcium Calculator™ created by registered dietitians working for the full term for BC Dairy Foundation in the 1980s.[16] The KCAT includes 7 food groups consisting of 24 categories with 45 food items containing calcium and vitamin D, which are consumed frequently by Koreans. Using the KCAT, dietary vitamin D as well as calcium intake can be assessed with excellent validity and reproducibility.[16] Low intake group for calcium was defined as <700 mg daily and low intake group for vitamin D as <10 µg daily in women ≥50 years of age.[14]
3. Risk factors for osteoporosis and fracture
Demographics including age, height, weight, body mass index (BMI), family history of osteoporosis, family history of osteoporotic fracture, status of residency (alone, with family, special facility), location of residence (urban and rural), status of insurance (Medicare and Medicaid), current smoking, comorbidity (hypertension, diabetes, hypercholesterolemia, rheumatoid arthritis, use of steroid) were evaluated.
BMD of the lumbar spine and femoral neck measured using a dual energy X-ray absorptiometry (DXA). Diagnosis of osteoporosis was made using the World Health Organization T-score criteria, with osteoporosis defined as a T-score ≤-2.5 at either the femoral neck or lumbar spine.
4. Statistical analyses
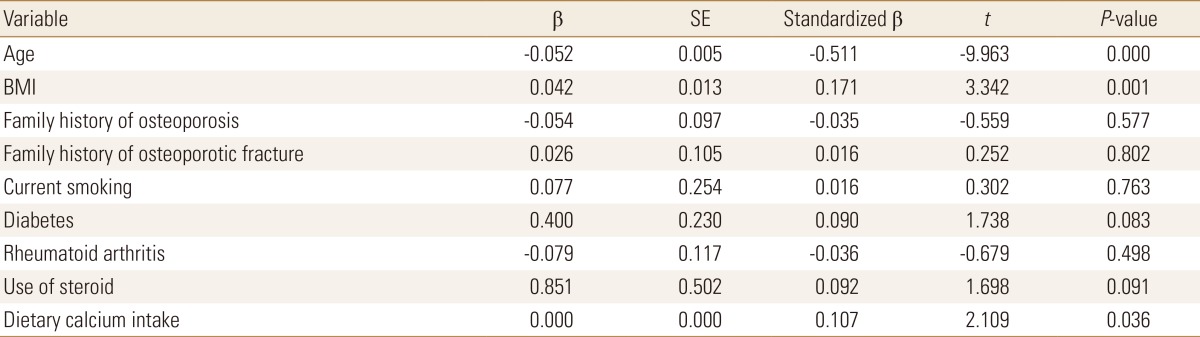
Analyses were performed using R software. Chi-square test and Student's t-test were used for comparison between low intake and adequate intake groups. To evaluate relationships and dependencies between calcium and vitamin D intake and T-score of femoral neck, Pearson's correlation and multiple regression analysis were used. The impact of calcium and vitamin D intake on BMD was evaluated with a multiple regression model. The covariates were age, BMI, family history of osteoporosis or osteoporotic fracture, use of steroids, current smoking, diabetes, and rheumatoid arthritis. The results were considered significant for P<0.05.
RESULTS
From January to July 2015, 277 women were enrolled. Mean age was 73.3 years old (range, 50-97 years). One hundred and forty-three patients (51.6%) were taking an osteoporosis medication. One hundred and eighteen patients (82.5%) were taking bisphosphonate and 14 patients (9.8%) were taking a selective estrogen receptor modulator. There were vertebral fracture in 32 patients, hip fracture in 195, and wrist fracture in 50. One hundred and seven patients (38.6%) had osteoporosis indicated by BMD.
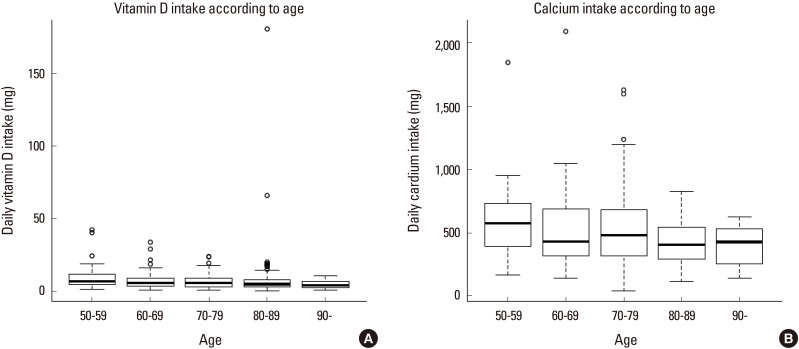
Calcium intake ranged from 36.4 to 2,090.8 mg daily, with a mean of 503.7±274.7 mg. Vitamin D intake ranged from 2.7 to 180.8 µg daily, with mean of 7.5±12.6 µg. Only 56 patients with osteoporotic fracture (20.2%) had a daily calcium intake above the recommended level of 700 mg. Two hundred and twenty one patients (79.8%) had a daily calcium intake <700 mg/day. Similarly, dietary vitamin D intake of 216 patients (78.0%) was <10 µg/daily. Only 19 patients (6.9 %) were taking calcium and vitamin D supplements. Figure 1 shows the daily calcium and vitamin D intake in each age group. Dietary calcium intake showed a decreasing tendency according to increasing age. However, there was no difference in vitamin D intake according to age group.
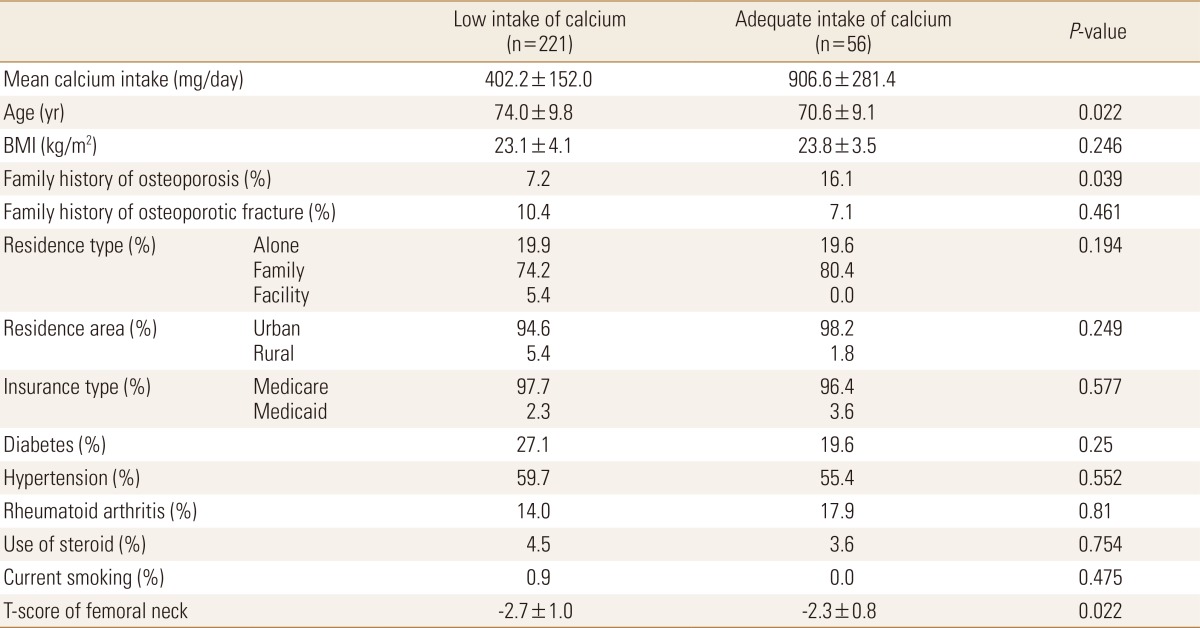
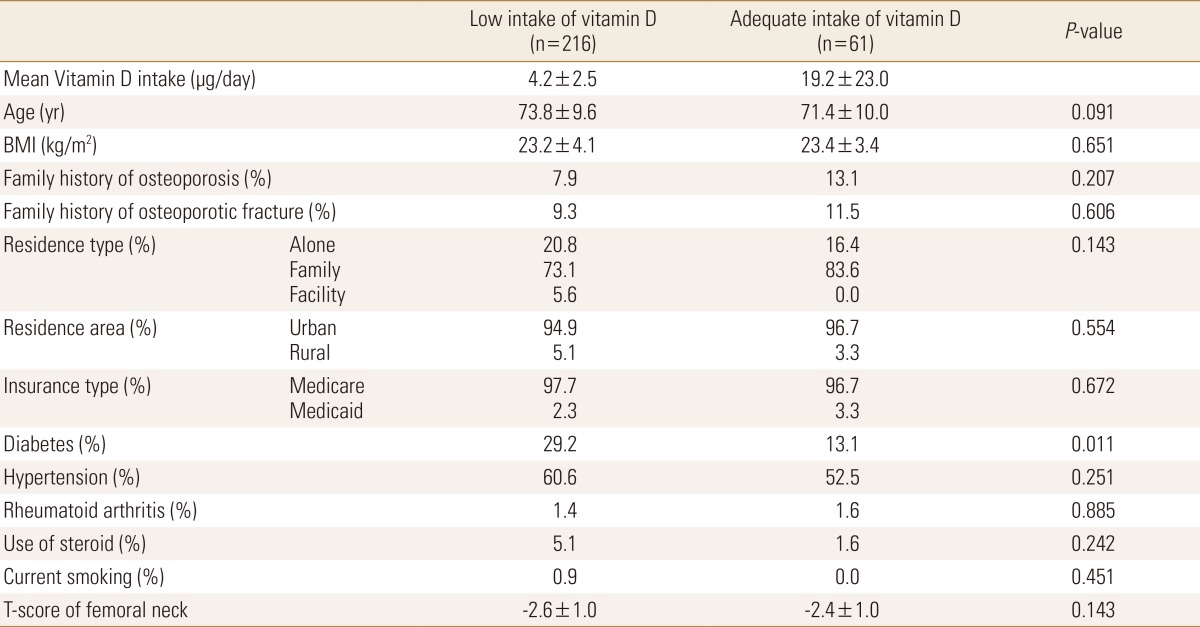
Patients with low dietary calcium intake were older (P=0.022), had less family history of osteoporosis (P=0.039), and had lower femoral neck BMD T-score (P=0.022) (Table 1). Diabetes was more prevalent in patients with low dietary vitamin D intake (P=0.011) (Table 2). There was no difference in femoral neck T-score in subjects with low and adequate intake of vitamin D.
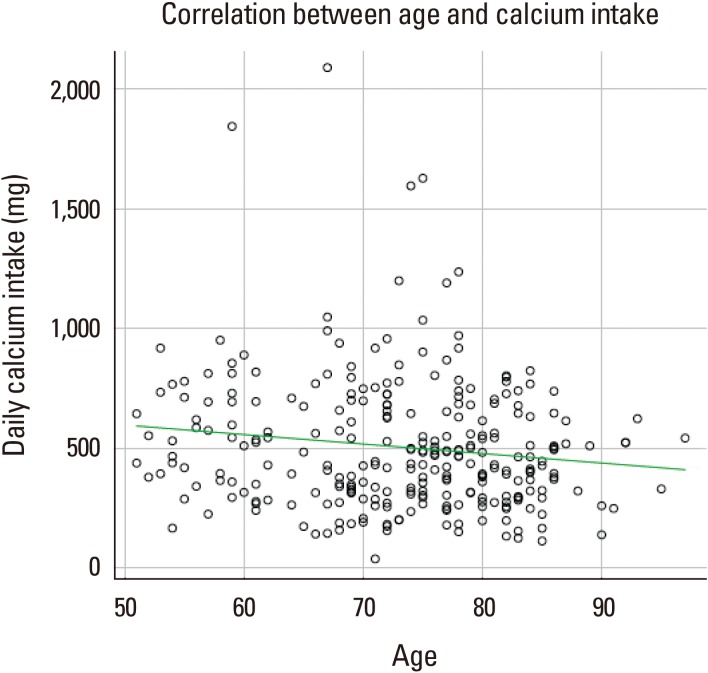
We studied the various possible predictors of low calcium and vitamin D intake including age, BMI, family history of osteoporosis or osteoporotic fracture, residence type and area, smoking, diabetes, hypertension, rheumatoid arthritis, and use of glucocorticoid. Significant correlation was evident between age and calcium intake (r=-0.14; P=0.019; Fig. 2). However, no correlating factors associated with vitamin D intake were evident; the correlation between vitamin D intake and age was statistically non-significant (r=-0.025; P=0.675).
BMD was determined in 31 patients with spine fracture and 182 patients with hip fracture. Among patients with hip fracture, 71 (37.0%) patients had hip T-scores in the osteopenic range and 111 (57.8%) patients had hip T-scores in the osteoporotic range. Among spine fracture patients, 16 (51.6%) patients had spine T-scores in the osteopenic ranges. When we applied spine or hip T-scores, 9 (22.6%) patents with spine fracture and 14 (7.7%) patients with hip fracture could be re-categorized from osteopenia to osteoporosis. In the multivariable model, age, BMI and calcium intake were significantly associated with T-score of femoral neck (Table 3). Vitamin D intake was not associated with T-score of femoral neck.
DISCUSSION
This study demonstrated high prevalence (about 80%) of low calcium and vitamin D intake in elderly Korean women with osteoporotic fracture. Older age and no family history of osteoporosis were associated with low calcium intake. In multivariate analysis, calcium intake showed a statistically significant association with femoral neck T-score.
Calcium plays an essential role in bone health across all ages, so calcium intake is emphasized because an insufficient intake negatively affects bone metabolism.[17]
Asian populations tend to have low calcium intake.[18,19] A recent cross-sectional study from Korea reported that the mean daily calcium intake was 485 mg in the general population ≥50 years of age.[20] According to national health statistics, more than 50% of general population at any age has a lower calcium intake than the KDRI recommendation. In this study, dietary calcium insufficiency was observed in 80% of patients with osteoporotic fractures. The prevalence of low calcium and low vitamin D intake in this study were higher than reported from other countries.[21,22,23,24] The average daily calcium intake in the diet is <500 mg, meaning that older people would need to take calcium supplements to meet the recommendations. In some Western countries, more than 30% to 50% of older women take calcium supplements.[25,26,27,28] In this study, only 7% of enrolled women were taking calcium or vitamin D supplements, which was lower than other previous studies. Given that participant in this study were at high risk of subsequent osteoporotic fracture, a systemic approach should be made to increase the dietary calcium intake after fracture.
In this study, factors affecting the calcium intake were age and family history of osteoporosis. Patients with family history of osteoporosis took more calcium. Awareness and concerns about osteoporosis could affect dietary habits in patients with family history of osteoporosis. As it has been confirmed in previous studies,[21,24] older women have lower calcium intake. Moreover, lower calcium intake showed a statistically significant association with lower femoral neck T-score, even after adjusting age. Recently, Kim et al.[29] also reported that low calcium intake was significantly related with low BMD and increased risk of osteoporosis in general population in Korea. Therefore, public education about the importance of adequate calcium and vitamin D intake is very important to prevent osteoporosis, especially in older women.
As vitamin D has been recognized as a critical factor in calcium metabolism, the effect of vitamin D on bone density has been reported.[21,30] However, we did not find any relation between vitamin D intake and BMD. Sun exposure is important as a non-dietary source of vitamin D. In this study, we did not measure serum 25-hydroxy-vitamin D (25-[OH]D), a well-known biomarker of vitamin D status, and did not investigate the time of outdoor activities. This suggests that dietary vitamin D intake alone may not accurately reflect the state of vitamin D in the body.
Our study has some limitation. First, this was a cross-sectional study. Prospective studies on the relationship between dietary calcium intake and bone are needed to determine whether these associations are causal. Second, data on the intake of each nutrient were provided as self-reporting questionnaire. Therefore, there is a possibility that the answer was incorrect considering the age of patient.
In conclusion, the results of this study show that the majority of patients with osteoporotic fracture had lower than recommended daily calcium and vitamin D intake. Therefore, all osteoporotic fracture patients would benefit from dietary education and calcium supplements to prevent bone loss and subsequent fracture.
 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Full text via PMC
Full text via PMC Download Citation
Download Citation Print
Print






