


INTRODUCTION
The World Health Organization (WHO) defines osteoporosis as a disease of the skeletal system characterized by abnormalities in the amount and architectural arrangement of bone tissue, resulting in an undue susceptibility to fractures, and the National Institute of Health (NIH) defines osteoporosis as a disease of the skeletal system in which the bones become weak and are more likely to break.[1] Based on the Korean National Health and Nutrition Examination Survey (KNHANES) in 2012, the prevalence of osteoporosis was 34.9% and 7.8% for females and males older than 50 years, which was thrice higher than the prevalence of osteoporosis in the United States as reported by the American National Health and Nutrition Examination Survey in 2013.[2]
Approximately 2.2 trillion dollars is spent each year on osteoporosis and related fractures in Korea, which is close to twice the amount spent on diabetes (Korea Centers for Disease Control and Prevention, 2011).[3] The recognition rate of osteoporosis is 24.7%, which means 3 of 4 patients with osteoporosis do not know they have osteoporosis. Only 10.8% of patients with osteoporosis, approximately 1 of 10, undergo treatment.[4] Therefore, promoting and regulating bone health are important among the general population.
The risk factors for osteoporosis include genetics, hormone,[5] exercise,[6] physical activity,[7] and nutrition.[8] Risk factors such as smoking, excessive alcohol consumption,[9] calcium deficiency, and vitamin D deficiency [10] can be corrected, and balanced nutrition influences bone mass and bone quality as well as fracture occurrence and treatment.[11] International researches reported that excessive sodium intake increases calcium excretion in the urine, which in turn decreases bone density.[12] Low calcium intake can increase osteoporosis risk,[13] and smoking is a relevant risk factor for osteoporosis.[14] Exercise and physical activities can affect bone density. Weight-bearing activities increase bone density, bone strength, and balance.[15]
Based on the information above, the Korean Society for Bone and Mineral Research provided recommended doses of drugs, meals, and other nutrients to prevent osteoporosis.[1] However, researches that support the recommended values are scarce. The present study's goal is to investigate the effects of correctable factors, such as life habits and nutrition by using the KNHANES. We were conducted to provide a basis for the national health guideline.
METHODS
1. Subject
This study was conducted by using the 2008 to 2011 KNHANES as raw data. Among the 37,753 initial subjects, subjects younger than 18 years (n=13,500), subjects who were pregnant or lactating, postmenopausal women, subjects older than 70 years (n=3,396), subjects without or missing bone density measurements (n=9,107), subjects with a history of fracture (n=510), subjects with low-caloric (less than 800 kcal) or high-caloric intake (more than 4000 kcal) (n=869), subjects with osteoporosis-associated diseases (diabetes, hyperthyroidism, renal failure, cirrhosis, rheumatism, and cancer) (n=2,203), subjects taking female hormone supplements (n=356), and subjects with missing variables (n=2,016) were excluded. The final analysis used the data from 3,419 subjects who were divided into the following three groups: normal (n=2,956), osteopenia (n=375), and osteoporosis groups (n=88) (Fig. 1).
2. Description of the parameter
The detailed variables used in the study were selected by using the KNHANES Guide from the examination and nutrition categories. The mean age, sex (male and female), body mass index, household income (low, middle-low, middle-high, and high), and educational level (below middle school graduate, high school graduate, above college graduate) were the demographic factors used to group the subjects.
Nutritional variables used in this study were appropriate intake of sodium, calcium, and protein. WHO recommends daily sodium intake less than 2 g, whereas the Korean Nutrition Society recommends daily and goal intake of 1.2 g and less than 2 g, respectively.[16] Therefore, this study used 2 g as reference to differentiate sufficient intake (less than 2 g per day) and excessive intake (more than 2 g per day). The evaluation of calcium intake was divided into sufficient and excessive intake by calculating the recommended intake to individual intake. The recommended intake for protein varies depending on age based on the Korean Nutrition Society. For example, adult men and women in their 30s are advised to consume 60 g/day and 50 g/day protein, respectively. These values were obtained by calculating the amount of protein that would satisfy the protein intake requirements of 97% to 98% of the sample population by using results from researches on nitrogen balance and protein digestion.[16] However, protein intake of Koreans are still excessive. Therefore, 0.8 g of protein intake per weight was used as reference to differentiate sufficient and excessive protein intake in this study.
Smoking and exercise were investigated as lifestyle-related variables. Subjects who currently smoking or previously smoking and those who have never smoking were included in the smoker and non-smoker groups, respectively. Subjects who intensive or moderate exercise more than thrice a week and those who intensive or moderate exercise less than thrice a week were included in the exercise and no-exercise groups, respectively.
3. Statistical analysis
All statistical analyses were performed using R 3.1.3 version freely available on the web (http://cran.r-project.org/) and SPSS (version 18.0; SPSS Inc., Chicago, IL, USA). Data were reported as mean±standard deviation (SD) or as numbers and percentages. The Chi-squared test and Kruskal-Wallis test was used to check if there are significant differences among the three groups. One-way analysis of variance (ANOVA) was conducted for bone status and various characteristics, respectively. If there seemed to be a significant differences, post hoc comparison was applied by Bonferroni's method. Odds ratio (ORs) were derived using multinomial logistic regression to estimate the association between bone health status and various factors. Adjusted ORs were derived after adjustment for the covariates. All results were considered statistically significant when P<0.05.
RESULTS
1. Demographic factors of the participants
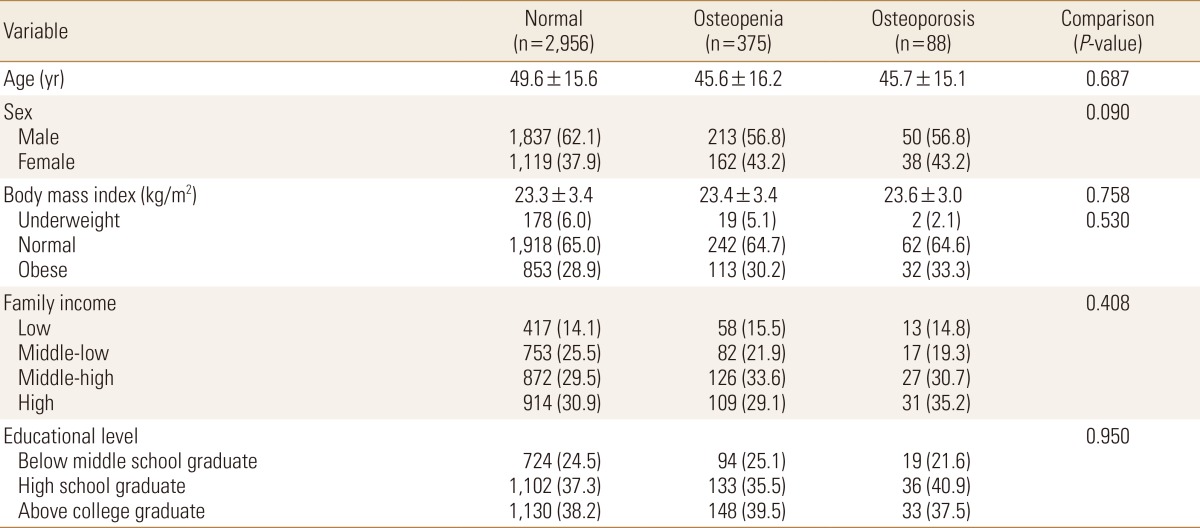
The proportion of the osteopenia and osteoporosis groups was 12.7% and 3.0%, respectively. The average age was 49.6 years, and the sex ratio showed that males were more than females. The proportion of overweight subjects increased with decreasing bone density, but the three groups showed no significant differences. Income level was similar in the three groups, which did not show any significant difference, and the educational level was also similar in the three groups for lower than middle school, high school graduate, and college graduate. Educational level showed no significant difference between three groups (Table 1).
2. Nutritional and lifestyle-related factors of the participants
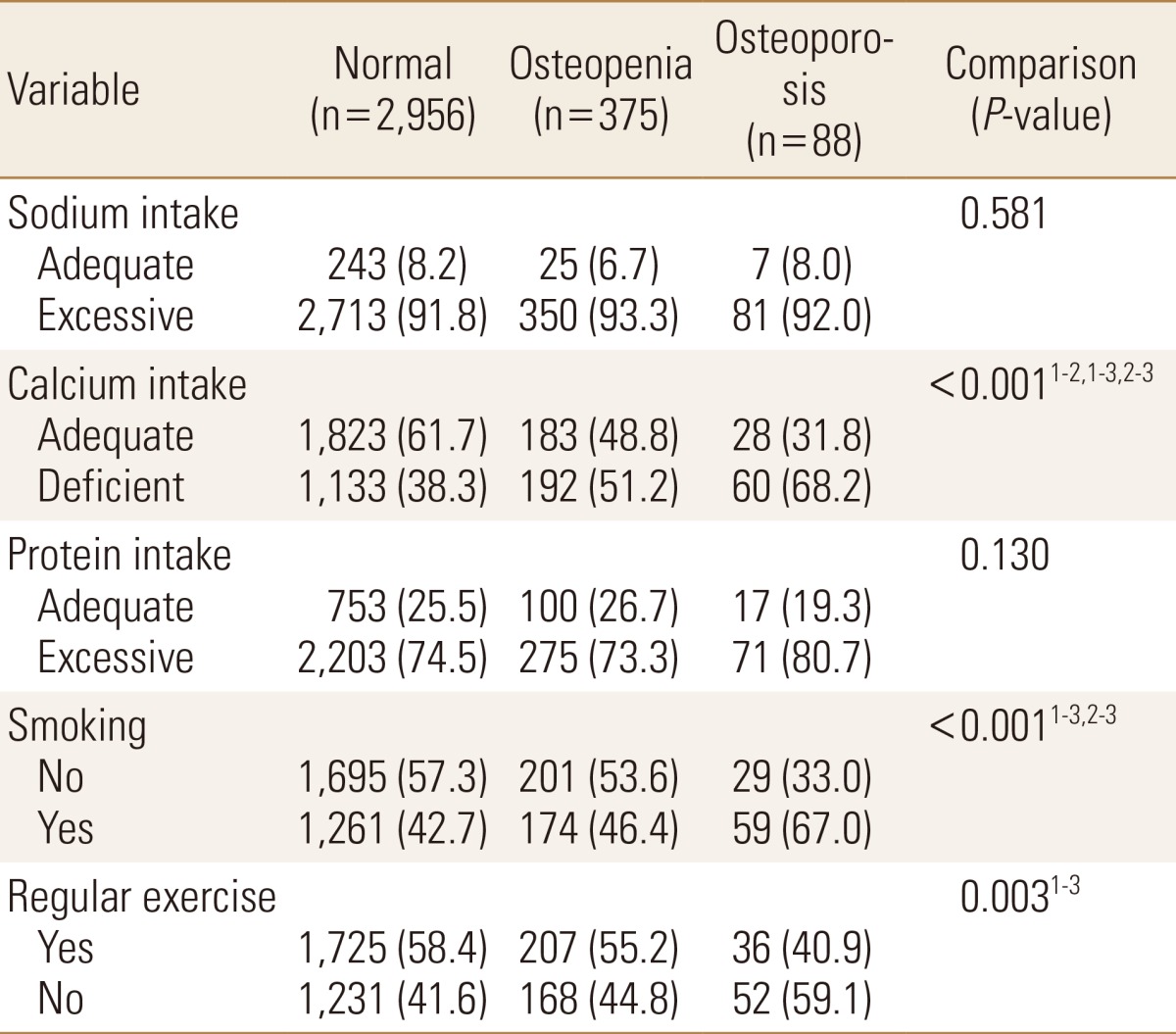
The sodium intake levels revealed that the proportion of subjects who consume excessive sodium were approximately 90% in all three groups. Calcium intake was deficient in 38.3% of the subjects in the normal group, whereas 51.2% and 68.2% of the subjects were calcium deficient in the osteopenia and osteoporosis groups, respectively. Adequate calcium intake showed significant differences in the three groups. The proportion of subjects who consume excessive protein was high in the osteoporosis group, but no significant difference was found between the three groups. The proportion of smoking was significantly higher in the osteoporosis group compared with the normal and osteopenia groups. The proportion of subjects who do not exercise was significantly higher in the osteoporosis group than in the normal group (Table 2).
3. Logistic regression analysis for bone health status
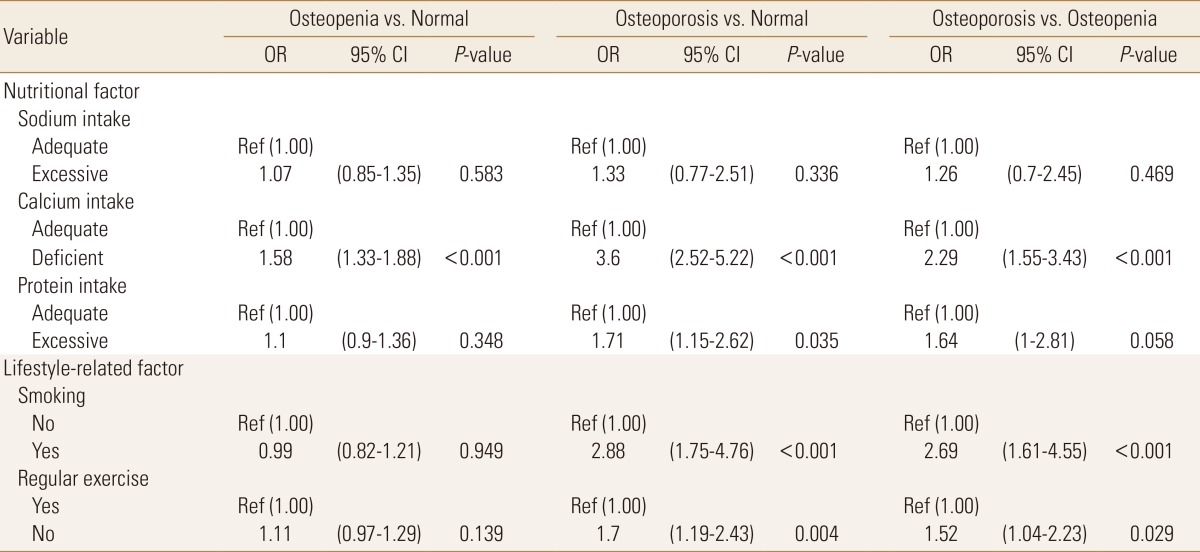
The factors showing the significant difference between three groups were analyzed by univariate logistic regression analysis for bone health status. Deficient intake of calcium was significantly associated with a threefold greater odds in osteoporosis group (OR 3.6; 95% confidence interval [CI] 2.52-5.22). OR was significantly increased in the osteopenia group compared to the normal group (OR 1.58; 95% CI 1.33-1.88). Excessive protein intake was significantly increased the risk only in osteoporosis group compared to the normal group (OR 1.71; 95% CI 1.15-2.62). When compared to "not smoking", smoking increased the risk in osteoporosis group compared to the normal group (OR 2.88; 95% CI 1.75-4.76), osteoporosis group compared to the osteopenia group (OR 2.69; 95% CI 1.61-4.55).When exercise was not performed, the risk increased in the osteoporosis group compared to the normal group (OR 1.70; 95% CI 1.19-2.43) (Table 3).
DISCUSSION
Several factors are known to affect bone formation or maintenance such as calcium, vitamin D, protein and other nutrients, physical activity, or disease. This study investigated the variables that affect bone density by using the factors provided by the KNHANES. The subjects were divided into three groups and compared. The social and economic factors were not significantly different between three groups. This study showed different results from previous studies, which identified sex and obesity as risk factors for osteoporosis. Nutritional and lifestyle-related factors showed that calcium deficiency, smoking, and lack of exercise were significantly different between the three groups, and regression analysis identified calcium as a strong factor closely related to the relative risk in all three groups. Based on the KNHANES in 2013, the average calcium intake of the Korean population was 70% of the recommended value.[17] Blood calcium levels are regulated by hormones. Continuous calcium deficiency depletes calcium within the bones, which is used for maintaining blood calcium levels, which increases the risk of osteoporosis. The study of Meleleo and Picciarelli [18] reported that calcium intake of more than 1,200 mg/day by incorporating dairy products in the diet of postmenopausal women for 1 year showed positive effects on bone density. Although many nutrients, such as vitamin D, magnesium, phosphorus, and vitamin K are necessary in bone formation, the guideline recommends a diet that lowers calcium excretion and improves absorption along with sufficient calcium intake. This study showed that calcium deficiency was prevalent in subjects with low bone mineral density. Calcium intake is crucial, and overall balanced nutrition is required to prevent and treat osteoporosis.
This study has several limitations. The number of subjects in each group are very different. In addition, the causality was difficult to be defined through the cross-sectional data. There may be recall bias. The use drugs, supplements of other nutrient and other were not considered. But importance of this study lies on the observation of correlation between the factors affecting bone density defined in the osteoporosis prevention and treatment guideline.
Recognition of an individual's self-condition and lifestyle-related management should be promoted and regulated to maintain bone health in the Korean population.

 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Full text via PMC
Full text via PMC Download Citation
Download Citation Print
Print






